Bon Secours Mercy Health to Outsource Home Health and Hospice to Compassus
Bon Secours Mercy Health (BSMH), the fifth-largest Catholic health system in the U.S., and Compassus, a leading national provider of home-based health care services, announced on May 2 that they have signed an agreement to form a 50/50 joint venture partnership for BSMH home care and hospice. Under the agreement, Bon Secours will outsource to Compassus, who will manage operations for 10 home health agencies and 11 hospice operations spanning five states.
Under the agreement, BSMH will maintain ownership of its existing hospice house real estate assets in specific locations while Compassus will manage the operations. BSMH will work closely with Compassus to support the home health and hospice associates transferring to employment with Compassus. Under the joint venture, the team will continue to provide spiritually grounded care and will operate in accordance with Ethical and Religious Directives.
The agreement is subject to state and federal regulatory review and final diligence; however, the agreement formalizes the intent of both parties to move forward with the transition and integration.
About Compassus
Compassus provides home-based services including home health, infusion therapy, palliative and hospice care. The company’s more than 6,000 team members serve more than 100,000 patients annually across more than 250 locations in 29 states. This is not the company’s first joint venture. In 2020, Compassus became managing partner of Ascension at Home, a joint venture between Ascension and Compassus.
About Bon Secours Mercy Health
Bon Secours Mercy Health (BSMH) is one of the 20 largest health systems in the United States and the fifth-largest Catholic health system in the country. The ministry’s quality, compassionate care is provided by more than 60,000 associates serving communities in Florida, Kentucky, Maryland, New York, Ohio, South Carolina and Virginia, as well as throughout Ireland.
Bon Secours Mercy Health provides care for patients more than 11 million times annually through its network of more than 1,200 care sites, which includes 48 hospitals. In 2022, BSMH provided more than $600 million dollars in community investments across five states, ensuring that cost is not a barrier to health care for patients in need.
In addition to charity care, BSMH invests in programs that address chronic illness, affordable housing, access to healthy food, education and wellness programs, transportation, workforce development and other social determinants of health. The Mission of Bon Secours Mercy Health is to extend the compassionate ministry of Jesus by improving the health and well-being of its communities and bring good help to those in need, especially people who are poor, dying and underserved. https://bsmhealth.org/
by Johnathan Eaves, Senior Director of Communications, Axxess
Treating Medicare patients comes with a level of nuance that is important to understand to ensure that organizations remain compliant and patients receive appropriate care. Standards for quality care and payment can sometimes be dictated by Medicare’s payment policies and at other times be decided by the Conditions of Participation. There is an important difference between these two governing principles that providers should understand to ensure compliance.
Care at home industry veteran and Axxess Senior Vice President of Clinical Services Arlene Maxim RN, HCS-C, offered insights into the differences between Medicare’s policy and its Conditions of Participation during a recent webinar.
Explaining the Difference
Maxim pointed out that the differences between policy and the conditional requirements comes down to what can be billed and what are the quality standards for the services provided.
“The Conditions of Participation are dealing primarily with quality, whereas Medicare policy is related to payment,” said Maxim. And while there is a difference, that doesn’t mean both aren’t important and must always be followed.
“If Medicare policies are not followed, you are audited and if you do not have documentation to support those policies, you’re not going to get paid,” said Maxim “Oftentimes, with PDGM, staff members are not getting past that first 30 days. They’re not understanding what they need to do to keep that patient who continues to qualify for services on for longer.”
Maxim says that the problem is often that clinicians do not understand Medicare policy. “Every piece of documentation we submit to the Medicare program for review [needs to be] as pristine as we can possibly get it,” she said.
Assessment and Documentation
Proper assessment and documentation is something Maxim feels is critical in ensuring quality care, meeting Medicare requirements, and receiving payment for services.
“Complete and detailed documentation is going to be the key for agency payment by the Medicare program,” Maxim said.
Maxim pointed out certain services covered under Medicare policy may include observation and assessment, management and evaluation of a care plan, maintenance therapy, teaching and training activities, administration of medications, wound care, ostomy care, rehab nursing, venipuncture, skilled nursing visits, and more.
She also cautioned that agencies need to be prudent with the funds they receive from Medicare, viewing them as a potential “short-term, interest-free loan” until undergoing any audit. Until their documentation is reviewed and approved, there are no guarantees.
“Medicare is an insurance and it’s not free,” said Maxim. “Medicare policy provides us with a list of covered items. If experiencing an audit, and if the documentation is not there to cover the covered service, you’re not in compliance with that Medicare policy and you will not be paid for the services.”
Communicating With Physicians
Maxim further emphasized the importance of frequent contact with physicians, adherence to care plans, and ensuring that care plans are simple with individualized plans and goals that are achievable.
“You want to make sure that you have orders that physicians are actually going to read and to determine that they make sense and they’re going to sign off on them,” said Maxim.
“Keep your plan of care simple.”
# # #
Axxess Home Health, a cloud-based home health software, streamlines operations for every department while improving patient outcomes.
By Beth Noyce, RN, BSJMC, BCHH-C, COQS CHAP-certified home health & hospice consultant
This is part 3 of the 3 in the series, outlining the discussions and implications in adopting new outcome and process measures for Hospice care. The final segment addresses future process and outcome measures that the board discussed, but did not yet implement. Read Part 1 on Outcome Measures and Part 2 on Process Measures.
The TEP discussed potential future process and outcome measure concepts that Abt Associates presented to the panel as well.
The process measures included:
Education for Medication Management
Wound Management Addressed in Plan of Care
Transfer of Health Information to Subsequent Provider
Transfer of Health Information to Patient/Family Caregiver
Hope-based outcome measures were:
Patient Preferences Followed throughout Hospice Stay
Hospitalization of Persons with Do-Not-Hospitalize Order
Developing education for medication management as a process measure was a popular concept, and the top priority of the recommended measures with the TEP as they “broadly agreed that CMS should develop this measure,” the report says, citing “a significant need for training in medication management for patients and their caregivers.” They recommended that the measure weigh more heavily when care is provided in a home setting than in a facility setting because hospices are unable to control facility training and hiring practices. One panelist commented that including the phrase “during today’s visit” in the measure is important.
Whether CMS should further develop the process measure addressing wound management in the plan of care was less straight-forward, as panelists provided varied feedback. They generally agreed that this measure is important, as having a record of wound management addressed in the plan of care can hold the staff accountable for treating the wounds. But some members recommended measuring wound management with outcome measures rather than process measures. One panelist cited potential problems from patients’ deterioration over time and another noted that the time frame of this measure is important, and encouraged recording the process of getting care in place once a wound is identified. The panel agreed CMS should carefully define the measure’s specifications.
Because standard practice for most agencies is, when a patient is discharged live, to transfer health information to the subsequent provider and to the patient and family or caregiver, TEP members expressed that the two measures were likely to “top out,” meaning they would almost always be marked “Yes,” making them of no value in differentiating between hospice providers. The group generally discouraged developing these process measures.
The group strongly rejected any merit in developing two outcome measures concerning Patient Preferences Followed Throughout Hospice Stay and Hospitalization of Persons with Do-Not-
Hospitalize Order. The report says “Multiple TEP members described situations in which patients who had preferred not to be hospitalized changed their minds when a crisis occurred. Patients’ preferences and unexpected crises are usually out of the hospice’s control. Although it is still important for hospices to ask patients about their preferences as part of patient-centered care, the TEP did not believe these two items would be practical measures of a hospice’s care quality.”
Dr. McNally expects that Abt. Associates will apply the HQEP TEP’s suggestions to the HOPE tool.
“Oh yeah, they did it,” he says. “Abt would come to a specific meeting with information, data, suggestions, and specific information about how these things would be measured. We’d give feedback. Then they’d come back to the next meeting having incorporated our suggestions,” he explains. “All of us felt very much heard and responded to. It didn’t feel in the least bit perfunctory.”
Whatever specific measures are eventually included in the HOPE tool, Lund Person sees value in its implementation. “Hospice providers have had a woeful lack of outcome measures for hospice patients, which has made the evaluation of quality hospice care based only on process measures and the family’s evaluation of hospice care in the CAHPS® Hospice Survey, she explains. “Implementing HOPE will begin to identify outcome measures that can be compared between providers.”
Lund Person warns of potential challenges as well. “The selection of risk adjustment and stratification must be carefully done to minimize bias and maximize effectiveness of measures,” she says. “In addition, hospice providers have been awaiting the release of the HOPE tool with significant anxiety about content and administrative burden.”
Dr. McNally is confident the HOPE tool will be a healthy change for hospices.
“A lot of my role as a medical director and hospice physician is supporting our nurses,” he says. “They do 95% of the work. I really would like to see this not be burdensome for our hospice nurses. I’m looking forward to seeing what the [HOPE tool] beta testing translates to in our own hospice world.” He added “What I would hope to see is that the tool feels user-friendly to the hospice team, the people who have to use it, and that it also provides useful information to patients and families.”
NAHC’s Wehri says that standardizing processes through the HOPE tool is the key foundational element for the hospice industry. “High quality care is driven by reducing variance through standardized processes, Wehri writes. “Also, CMS will have a better idea of how the type of population a hospice serves impacts some of the clinical care.” This small glimpse into hospice variances that CMS does not currently have could be very helpful in future policy and payment decisions, according to Wehri. “What CMS finds in terms of differences between hospices and their care for patients may be a bit of a surprise to CMS,” she says. “I hope they are pleasantly surprised with the overall quality of care that is revealed.”
# # #
Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.
DALLAS, April 25, 2024 – Axxess’ AGILE 2024 conference was a resounding success, with an unprecedented number of industry leaders, innovators and professionals coming together to explore the latest trends, exchange ideas and foster collaboration.
More than 50 partners supported AGILE (Axxess Growth, Innovation and Leadership Experience) with sponsorships of the three-day event, which attracted several hundred industry leaders, including C-suite executives, clinical leaders, operational and financial managers, industry investors and strategic advisors.
“The AGILE conference exemplifies our commitment to fostering growth, driving innovation and empowering leaders as we revolutionize the healthcare industry and pave the way for a future where quality care thrives in the confines and comfort of our homes,” said John Olajide, founder and CEO of Axxess, the leader in technology supporting care at home providers. “The feedback we’ve received on this year’s conference is truly inspiring, and we are already hard at work to make next year’s event a transformative experience, introducing new dimensions of knowledge, collaboration and inspiration.”
The conference formally began with a keynote address from healthcare innovator and futurist Nick Webb, who spoke on megatrends impacting the care at home industry, from emerging technologies to patient experience and staffing.
“The experience always wins,” he told the audience. “Patients and their families want friction freedom, they want speed, they want transparency, they want genuine, authentic empathy, they want this to be painless.”
The event included a day-long Leadership Forum attended by industry leaders who participated in high-level conversations about business operations, advocacy and insights on the state of mergers and acquisitions with key leaders in care at home, finance and public policy.
The value of technology was emphasized in a later panel discussion on embracing risk to reimagine healthcare, featuring Kim King, CEO of Home Care Network.
“We’ve found arming our staff with technology that allows them to do a virtual visit allows an aide to work at the high end of what they’re able to do so that they can give real information back to a clinician,” King said. “If we need to take it to the next step and get a virtual visit with a physician [or] arrange transportation to get somewhere, that makes all the difference in the world.”
Annie Erstling, Chief Operating Officer at Forcura, urged attendees to rethink their relationship with technology companies.
“You should lean on your technology partners,” Erstling said. “They should be real partners and they should keep you abreast of what’s the latest and greatest.”
Along with keynote speakers, panels and industry-specific education sessions offering continuing education credits, AGILE also included an Innovation Showcase featuring the latest developments to improve operations from Axxess partners, a GUIDE to dementia, which enabled participants to experience what those living with dementia go through each day, and a CPR training course where participants learned how to properly perform life-saving, hands-only CPR.
# # #
About Axxess
Axxess is the leading global technology innovator for healthcare at home, focused on solving the most complex industry challenges. Trusted by more than 9,000 organizations that serve more than 5 million patients worldwide, Axxess offers a complete suite of easy-to-use software solutions that empower home health, home care, hospice, and palliative providers to make healthcare in the home human again. Multiple independent certifications have confirmed that Axxess has the most secure and industry-compliant software available for providers. The company’s collaborative culture focused on innovation and excellence is recognized nationally as a “Best Place to Work.”
by Beth Noyce, RN, BSJMC, HCS-C, BCHH-C, COQS CHAP-certified home health & hospice consultant
Process Measures
The outcome measures being considered look at effectiveness of hospice clinical efforts to decrease pain and other symptoms. The process measures paired with them focus on the hospice’s follow up with the patient after moderate or severe symptoms are found during assessment.
Exhibit 6 (below) shows the numerator and denominator for these.
TEP members determined that these two process measures have high face validity. This means the measure items clearly state, or “look like” they will measure what CMS intends them to measure. This allows consumers to see what hospices are assessing and treating. It can also help hospices track how well they are reducing or treating patients’ symptoms.
Katie Wehri, Director of Home Health & Hospice Regulatory Affairs for the National Association for Home Care & Hospice says the face validity of process items is the most important information the HQRP TEP provided to CMS. “Having HOPE items and subsequent measures that actually measure what is intended is key to success,” she says.
Exclusions from Process Measures Success
Exclusions from calculating a hospice’s process measures’ success need careful consideration. Here is the list of options of which patients to exclude:
Patient desired tolerance level for symptoms
Patient preferences for symptom management
Neuropathic pain
Actively Dying (death is imminent)
Other conditions
The report says that reassessing a symptom within two days of identifying that symptom as moderate or severe is fundamental. This is true regardless of the beneficiary’s stated tolerance-level for symptoms. It also said that process measure calculations should include patients with no symptom-management preference. Further, exclusion criteria should be the same for pain and non-pain symptoms.
Neuropathic Pain
The TEP’s recommends including neuropathic pain in the HOPE tool’s pain-reassessment process measure. Including rather than excluding patients suffering neuropathic pain prompts nurses to reassess these patients for changes. The report references research that suggests 40% of hospice patients may experience neuropathic pain. Patients who experience neuropathic pain have more severe and more distressing pain symptoms. [Tofthagen, C., Visovsky, C., Dominic, S., & McMillan, S. (2019). Neuropathic symptoms, physical and emotional well-being, and quality of life at the end of life. Supportive Care in Cancer, 27(9), 3357-3364. doi:10.1007/s00520-018-4627-x]
The TEP agrees that patients with neuropathic pain should be part of the process measure. However, they recommend excluding the same patients from the outcome measure addressing the patient’s pain impact. The report cited TEP discussion that such pain is chronic and not likely to be resolved or decreased within two days when the reassessment captures outcome data.
The TEP broadly agreed that a nurse who assesses a patient who is actively dying (life expectancy of 3 days or fewer based on clinicians’ assessment) as suffering moderate or severe pain should attempt to reassess the patient. Such patientsshould not be excluded.
The panelists agreed that process measures should include patients of all ages. Several TEP members noted that all patients experience pain and non-pain symptoms, and therefore the measures should apply to adults and children alike.
Exclusion Due to Inability to Reassess
When a hospice is unable to reassess a patient for a valid reason process measures should exclude those patients.
Identified exclusion reason were:
discharge, alive or dead
visit refusal
inability to access the patient due to an emergency department or hospitalization event
the patient traveling outside of the hospice’s service area
inability of the hospice to contact the patient or caregiver.
However, the report says, “…hospices should be penalized if reassessment is missing or delayed due to hospice staffing or scheduling issues.”
This article is the second in a series about implementation of HOPE. Next week, Beth Noyce shares details from the panel as it discussed potential future process and outcome measure concepts.
HHAeXchange Names Scott Schwartz as Chief Operating Officer, Announces New Senior Vice President of Product
New appointments highlight the company’s commitment to equipping providers, managed care organizations (MCOs), and state Medicaid agencies with solutions that enable more effective homecare
NEW YORK, Feb. 21, 2024 – HHAeXchange, a leading provider of homecare management solutions for providers, managed care organizations (MCOs), and state Medicaid agencies, today announced that Scott Schwartz, formerly Chief Revenue Officer, has been appointed to Chief Operating Officer, and Lori Harrington has joined the team as Senior Vice President of Product.
After serving as Chief Revenue Officer, Senior Vice President, and Vice President of Sales & Marketing at HHAeXchange for nearly seven years, Scott Schwartz will step into a new role as Chief Operating Officer. In his new position, Schwartz will lead implementation, revenue cycle operations, integrations, technical customer care, training, and customer education. Bringing these functions under Schwartz’s leadership will evolve operations to enable more effective services and solutions.
“Over the past seven years, Scott has been integral in establishing HHAeXchange as the leader in homecare software through helping nearly 10,000 homecare provider agencies leverage technology and spearheading our robust Partner Connect program,” said Paul Joiner, Chief Executive Officer at HHAeXchange. “As we work to expand our platform and create better solutions for homecare providers and payers, Scott’s top priority will be driving operational excellence and delivering an improved end-to-end client experience.”
In addition to the appointment of Schwartz as COO, the company has announced Lori Harrington as the new Senior Vice President of Product. With over twenty years of experience in the industry, Harrington brings an extensive healthcare product strategy and management background to the organization. In her most recent role, Harrington served as Vice President of Product Management for Teladoc, where she led product strategy for value-based care initiatives and was instrumental in developing a client innovation hub for strategic health plan clients, creating a streamlined experience for clients based on their emerging needs.
“Lori’s deep understanding of healthcare and her customer-centric approach will be crucial in advancing our product solutions to serve providers and payers better,” said Tim Brewer, Chief Technology Officer at HHAeXchange. “With her vast experience, Lori will play a pivotal role in driving product evolution and execution, improvements to our current products, and delivering solutions that meet the evolving demands of our customers and the homecare industry to ultimately provide better customer satisfaction.”
As aging populations across the country continue to increase and more members express a preference for homecare, these new appointments will advance HHAeXchange’s commitment to setting new industry standards that enable providers, caregivers, payers, and families to deliver the best care in the home.
Founded in 2008, HHAeXchange is the leading technology platform for homecare and self-direction program management. Developed specifically for Medicaid home and community-based services (HCBS), HHAeXchange connects state agencies, managed care organizations, providers, and caregivers through its intuitive web-based platform, enabling unparalleled communication, transparency, efficiency, and compliance. To learn more information, visit hhaexchange.com or follow the company on Twitter, LinkedIn and Facebook.
By Beth Noyce, RN, BSJMC, HCS-C, BCHH-C, COQS Home health & hospice consultant
The Hospice Outcome Patient Evaluation is a step closer to implementation.
After four years of considering options, the Technical Expert Panel (TEP) has finished its work that will inform future Hospice Quality Reporting Program results. The TEP considered quality measures to include in hospice’s future assessment tool and best choices for risk adjustment and exclusion.
The panel convened in 2019 “[we are] committed to improving the quality of care given to hospice patients,” says the 2022-2023 TEP Summary Report: Hospice Quality Reporting Program. The panel aimed to ensure that hospice quality measures are meaningful for hospice beneficiaries, transparent to hospice providers, and useful to consumers. They considered quality measures from both HOPE and claims data.
“From day one it was very clear Medicare wanted to make this a very different experience for hospice teams and make it a more valuable thing for consumers,” says Dr. Jeff McNally, Hospice Medical Director at Utah’s Intermountain Hospice,” describing his participation on the HQRP TEP. “I was actually encouraged and inspired by it,” he says. “It was the first time I had first-hand experience working with any kind of CMS entity.
“The reality is some clinicians in the field and leaders don’t have the best things to say about CMS,” he explains, but “whatever we were considering we always circled back to whether it would be burdensome to the clinical team and would it be valuable to consumers.”
The panel initially planned to meet multiple times in person, with two meetings per year and potential virtual meetings as needed. “Then COVID hit,” Dr. McNally says. “It slowed the process considerably. We never did meet again in person.”
The HQRP TEP met eight times over four years, virtually after the initial meeting. McNally described participants as coming to each meeting prepared with data and proposals for HOPE measures for which they would request input from panelists.”
From TEP recommendations early in their work, Abt Associates developed two outcome measures and two process measures in harmony with hospice’s central tenet to manage symptoms:
Process measures:
Timely Reassessment of Pain Impact
Timely Reassessment of Non-Pain Symptom Impact
Outcome measures:
Timely Reduction of Pain Symptom Impact
Timely Reduction of Non-Pain Symptom Impact
“The most important [recommendations] were some of the outcome measures about symptom management,” McNally explains. “What should we be helping agencies show that they’re doing well? And how do we do that? Deciding which ones, and how many symptom management measures to use and the most valuable way to show it in a fair way.”
During the past two years, TEP members prioritized which of the risk-adjustment factors suggested by Abt. Associates should apply to outcome measures and which exclusions should apply to both outcome and process measures.
The report describes risk adjustment as using statistics to exclude “confounding factors,” or elements that are outside of a hospice’s control, from calculations that could make a hospice’s performance appear either better or worse than it is. In essence, risk adjustment increases the fairness in outcome-measure calculations while exclusions do the same for both outcome and process measures.
For the outcome measures being considered, the report says that the “TEP broadly agreed that risk adjustment is very important because it accounts for external factors outside hospices’ control and more accurately reflects the quality of care provided.”
Judi Lund Person, Principal of LundPerson & Associates, LLC, agrees. “The discussion of risk-adjustment factors is vitally important to the success of upcoming process measure implementation,” says Lund Person.
Determining which risk-adjustment factors to bring to the table was not easy. “There were some nuance things that we hashed out to try and decide how to weigh some factors in risk adjustment” for outcome measures, McNally explains.
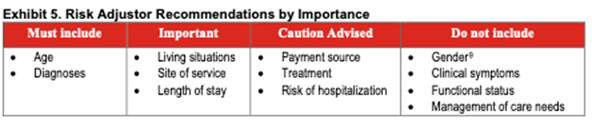
Exhibit 5 (below) summarizes the TEP’s rankings of risk adjustors suggested.
While the TEP’s priorities seem clear, the discussion concerning each risk adjustor was more complex. The TEP broadly agreed that the most important risk-adjustment factors are age and diagnosis. Some diseases are more difficult to manage than others, and patient condition tends to decline with age regardless of provider activity. Therefore, the TEP recommended that CMS adjust for these factors to ensure that common external factors do not adversely affect reported hospice care quality.
Here’s part of the nuance – the TEP also raised concerns that how well other patients with certain diseases or of certain age groups are treated might be valuable to some patients and their families seeking care for someone of the same age group or condition. Panelists fretted over possibly obscuring that information for consumers seeking hospice care by adjusting for those risk factors.
Living situation as a risk adjustor ranked as important to TEP members because hospices have no control over what level of assistance is available to patients. Similarly, site of service ranked high as a risk adjustor because, said some panelists, care is delivered very differently across settings, and patients and/or caregivers tend to provide higher hospice satisfaction ratings for hospices in home settings than for those in facilities,” according to the report.
Lund Person, who is also former Vice President of Regulatory and Compliance at the National Hospice and Palliative Care Organization (NHPCO), notes that the TEP recognized living situation and site of service as “important” risk adjustment recommendations.
“Identifying site of service will help to distinguish between care at home and care in a facility,” she says. Also vital, she continues, “is the recommendation from the TEP to consider length-of-stay as a risk-adjustment factor, including the differences between a 4-day length of stay and a 6-month length of stay.”
One TEP member cautioned that using payment sources, IV therapy, and risk of hospitalization as risk adjustors might tempt some hospices to use them to distort a hospices’ apparent care quality.
TEP members did not recommend using as risk adjustors gender, clinical symptoms, functional status and management of care needs. They did not discuss why they rejected gender, but several agreed that using clinical symptoms would not be of value because of their high correlation with diagnoses. Because hospice providers typically see hospice patients decline in ADL and IADL abilities, and hospice goals are focused on comfort rather than functional improvement, functional status was on the TEP’s “Do Not Include” as a risk adjustor list. And finally, one TEP member strongly opposed adjusting for patients’ medication management, supervision or safety assistance needs (management of care needs), explaining that “the public and CMS should hold hospices accountable for planning around oral medication, injectable medication management, and supervision and safety assistance,” the report says.
The TEP did suggest that using some risk adjustment factors as part of the HQRP could assist hospices internally with quality improvement while others would be more valuable to patients and families. For example, Patients and families would benefit from more straightforward risk adjustment that helps them select a hospice,” the report says, “including factors such as diagnosis. For publicly reported data used to select a hospice, the TEP suggested using demographic factors (including age but excluding gender), socioeconomic factors, living situation, and diagnoses.”
Dr. McNally hopes eventually to use HPRP data to promote Intermountain Hospice’s care. Intermountain Hospice is part of Intermountain Health, a health care provider with presence in multiple states. “You can’t take the current metrics to doctors’ offices and families to show anything meaningful,” he says. “It’d be great to have metrics we could take to our neurology docs and other docs,” he says. “I really think we provide better care and more options when patients stay within our system.
This article is the first in a series about implementation of HOPE. Next week, Beth Noyce shares details from the panel as it evaluated process measures.
HealthRev Partners Launches Velocity as a SAAS, Transforming Revenue Cycle Management for the Home Health and Hospice Industry
Meta: Discover how HealthRev Partners’ innovative SAAS solution, Velocity, is transforming revenue cycle management in the healthcare industry. Gain insights into its key advantages, AI capabilities, and data exchange interface engine feature set. Learn how Velocity empowers agencies with transparency, efficiency, scalability, and security to enhance profitability and operational excellence. Contact HealthRev Partners for a demo and revolutionize your revenue cycle management today.
Ozark, MO – April 1st, 2024 – HealthRev Partners, a leading innovator in healthcare technology, has announced the launch of Velocity as a Software as a Service (SAAS), revolutionizing revenue cycle management in the home health, hospice, and palliative care industries. This game-changing solution is designed to transform revenue cycle management (RCM) for multi-site agencies. In an era where the aging population in America increasingly desires to age in place, mergers and acquisitions in the home health space are driving the necessity for centralized data and operational processes. The trend of overseas hiring to reduce costs has created gaps in insights, emphasizing the critical need for real-time data to impact care promptly.
Michael Greenlee, Founder and CEO of HealthRev Partners, expressed his enthusiasm about the launch, stating, “Velocity as a SAAS represents a significant leap forward in revenue cycle management technology. By offering agencies unprecedented insights into their operations and empowering them with tools for optimization and growth, HealthRev Partners is setting a new standard in RCM solutions.”
Empowering Multi-Site Agencies and Enhancing Management Insights
As multi-site agencies navigate the complexities of managing diverse locations and teams, the demand for comprehensive insights and seamless integration becomes critical. HealthRev Partners recognizes this challenge and introduces Velocity as a SAAS to address the evolving needs of growing agencies. With a focus on providing real-time analytics and enhancing operational efficiency, Velocity bridges the gap between disparate locations and centralizes data for streamlined management.
Seamless Integration with Any EHR System
A key component of Velocity is the data exchange interface engine feature set. The ability to connect, integrate, translate, and import financial, claims, coding, clinical, operational, EHR, clearinghouse, and diverse data sets is vital for any organization. Velocity uses its proprietary interface technology engine along with robotic processing technology (RPA) to connect all disparate data sets within Velocity resulting in actionable data at your fingertips.
AI Capabilities to Increase Coding Accuracy
Velocity harnesses AI capabilities to automatically assign charts to coding professionals, enhancing efficiency and accuracy. By leveraging artificial intelligence, it streamlines the ICD-10 coding process and provides intelligent suggestions for selecting codes at the highest level of specificity to maximize reimbursement. Additionally, it utilizes advanced algorithms to analyze data and offer insights into PDGM-approved primary codes and comorbidity adjustment categories. Furthermore, Velocity’s AI-driven system assists in risk and comorbidity adjustments by recommending compatible code combinations and presenting primary and secondary code sets to facilitate precise coding decisions.
Key Advantages of Velocity:
Increased Transparency and Visibility: Real-time insights into all aspects of the revenue cycle across multiple sites. Identify bottlenecks, track productivity, and optimize operations seamlessly.
Enhanced Efficiency and Accuracy: Streamlined processes and standardized procedures that ensure consistency across all locations. Improve accuracy in coding, claim submission, and reimbursement.
Improved Communication and Collaboration: Facilitate real-time data sharing between clinical, financial, and operational teams at different sites. Enhance collaboration and decision-making.
Scalability and Security: Easily scale operations to accommodate growth needs while maintaining top-tier data security standards. Ensure compliance with regulatory requirements across all locations.
Michelle Mullins, MHA, BSN, RN – Partner & Chief Operating Officer of HealthRev Partners, highlighted the transformative impact of Velocity by stating, “Velocity illuminates your RCM’s path to predictable revenue. It empowers agencies with granular insights, customizable control, streamlined operations, and trustworthy security. This tool is not just a solution; it’s a revolution in revenue cycle management.”
The launch of Velocity as a SAAS marks a pivotal moment for agencies seeking to optimize their revenue cycle processes. With its focus on transparency, efficiency, communication, scalability, and security features, Velocity is poised to reshape how agencies manage their RCM operations.
# # #
For more information about Velocity as a SAAS or to schedule a demo, visit HealthRev Partners’ website.https://healthrevpartners.com/
by Bryan Robinson, PH.D. Contributor author of Chained to the Desk in a Hybrid World: A Guide to Balance
April is National Stress Awareness Month with the goal of raising awareness of the impacts of stress. According to the American Psychiatric Association, 26% of respondents anticipate they will be more stressed in 2023 and their mental health will be worse. Two out of five adults ranked their mental health from “fair” to “poor.” When you have fewer stressors, you have increased emotional stability, better moods and overall superior health. This month is a time to pay special attention to how you can remain stress-free throughout your workday, and you can do that in very simple ways. You don’t have to quit your day job or even work fewer hours. You can continue your daily work routines while practicing stress reducers at the same time. The one thing you must do is have a stress awareness plan that you can practice at work.
A Stress Awareness Plan Keeps Job Stress At Bay
My 2023 New Years Resolution was to do one kind thing each day for someone—especially strangers. It has heightened my awareness of how important and easy it is to be kind to others without taking extra time. Plus, how simple it is to practice and how good it makes me feel (and hopefully the other person) in just minutes. A work stress awareness plan has the same effect. Here’s how it works. Simply choose one thing to commit to each day that you can accomplish in three to five minutes to mitigate stress during your workday.
A max of five minutes of chill a day can have mental and physical benefits to keep you engaged, calm and energized on the job. These short work breaks lead to higher job engagement and performance as well as better sleep, increased immunity, lower blood pressure, improved digestion and increased emotional well-being. In fact, research from scientists at North Carolina State University shows the value of what I call Microchillers or taking what the researchers call Microbreaks throughout the workday. These short breaks—I recommend five minutes or less—are effective energy management strategies as simple as stretching, walking up and down stairs, gazing out a window at nature, snacking or having a five minute mindful meditation.
Viventium Releases its 2024 Caregiver Onboarding Experience Report, Demonstrating a Need to Raise the Bar for Onboarding in the Post-Acute Care Industry
BERKELEY HEIGHTS, N.J., April 02, 2024 (GLOBE NEWSWIRE) — Viventium, the leading SaaS-based human capital management platform serving the post-acute care industry, released its 2024 Caregiver Onboarding Experience Report, a comprehensive research study analyzing survey responses from 175 post-acute care administrators and 220 caregivers. The report finds a shockingly low bar for what passes as a “good” onboarding experience in home-based and facility/community-based care, with strong indications that raising that bar could correlate to higher retention rates.
“Staffing shortages and high turnover rates within post-acute care are recurring issues in need of solutions,” said Navin Gupta, Viventium CEO. “Our research illuminates a crucial pathway towards addressing these persistent challenges, and it begins with onboarding.”
Findings point to post-acute care managers and administrators having a major impact on the steps their organization can take to better engage, motivate, and retain its caregiving staff.
“The study significantly advances our knowledge of what it takes to recruit and retain caregivers in today’s highly competitive workforce market. The onboarding process is fully within the control of the employer, and the study shows that doing it right pays dividends. Most notably, many of the elements of successful onboarding are simple improvements in the process that bring a real return on investment. I would encourage all of home care to learn from this study.”
About Viventium
Viventium provides a SaaS-based human capital management solution that is focused on the post-acute care industry. The company’s mission is to enrich the lives of caregivers through technology so they love going to work every day. By providing specialized software and expert guidance, Viventium helps its clients throughout the lifecycle of each caregiver. The company has clients in all 50 states and supports over 420,000 client employees each year.
 Compassus provides home-based services including home health, infusion therapy, palliative and hospice care. The company’s more than 6,000 team members serve more than 100,000 patients annually across more than 250 locations in 29 states. This is not the company’s first joint venture. In 2020, Compassus became managing partner of Ascension at Home, a joint venture between Ascension and Compassus.
Compassus provides home-based services including home health, infusion therapy, palliative and hospice care. The company’s more than 6,000 team members serve more than 100,000 patients annually across more than 250 locations in 29 states. This is not the company’s first joint venture. In 2020, Compassus became managing partner of Ascension at Home, a joint venture between Ascension and Compassus. , compassionate care is provided by more than 60,000 associates serving communities in Florida, Kentucky, Maryland, New York, Ohio, South Carolina and Virginia, as well as throughout Ireland.
, compassionate care is provided by more than 60,000 associates serving communities in Florida, Kentucky, Maryland, New York, Ohio, South Carolina and Virginia, as well as throughout Ireland.
 Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.
Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.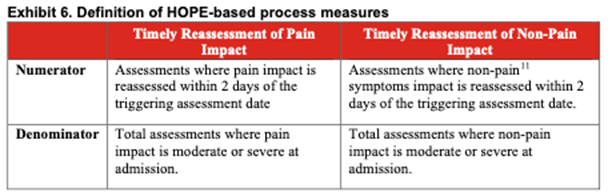

 April is
April is 
