by Tim Rowan | Oct 9, 2025 | Admin, Medicaid, Product Review, Waste Fraud and Abuse
by Tim Rowan, Editor Emeritus
Software Eliminates Fraud and Errors
Like so many Home Care providers, Aspen Home Care in Kansas City, Missouri was drowning in paper. Two hundred caregivers turned in weekly timesheets every Friday. A large office staff had to go through them, looking for errors, omissions, and unauthorized visits and shifts. Submitting erroneous claims, of course, leads to payment denials, even fines. When an agency submits too many bad claims every week over a long period, a surveyor will soon be knocking at their door.
On a good week, Aspen completed all necessary payroll and billing tasks and had bills ready to submit by end of business on the following Thursday. Slowing down the process were the usual errors — forgotten check-outs, more hours worked than authorized, and late timesheet submission. Caregivers grew weary of the weekly phone calls asking for clarification, even when the error was their fault. Aspen did have a basic billing system, but paper timesheets fed it too. Electronic Visit Verification was possible, but only via a patient’s landline, using punched-in identification codes.
“After years of software design, we have completed our replacement for your billing and EVV system. We would like you to switch from the basic system we sold you a few years ago and beta test our better one.”
– Henry (Hank) Schwab, Owner, Compliance Plus
Beta testing is a risky venture, but both owner Ahmed Jara and Office Manager Mohammed Mohammed* trusted Hank and agreed to give it a try. After all, the agency was drowning in paper, they reminded each other.
Dramatic Process Improvements
We took part in a demo of the Compliance Plus system before speaking with Mohammed and hearing Aspen’s experience. We saw a comprehensive, user-friendly system, with a color-coded user interface, that includes scheduling, EVV, and billing for Medicaid, Managed Care, and all other payers an agency contracts with.
Caregivers clock in and out with an app that is GPS-enabled down to exact longitude and latitude coordinates. Should a patient live in an internet dead zone, caregivers can use their landline. If there is no landline, Aspen will install a “smart fob” in the home. Aspen does not require specific visit start times, but once a check-in is recorded, the app knows the patient’s authorized hours and automatically alerts the caregiver when it is time to clock out.
Mistakes do happen, of course, but fixing them is not difficult. When the Compliance Plus back end sees a 14-hour visit, it assumes the caregiver forgot to check out. The visit flashes red on the screen, indicating it is not ready to bill, and displays the difference between authorized and recorded hours. The office employee managing exceptions simply calls the caregiver for verification and then manually edits the end time, and compliance is maintained.
Mohammed told us his caregiving staff is thrilled with the app, though he did say the transition was hard at first. “They learn to use it in about 30 minutes,” he said. “Check-in and check-in take a few seconds and now they are happy to be done with paper forever, not to mention no longer having to deliver paper timesheets to the office.” He added that fake check-ins from the car on the way to a patient’s home have been completely eliminated.
Most importantly, the three-person office staff now completes payroll and billing for 200 caregivers by midday on Tuesday instead of late on Thursday.
The "Plus" of Compliance Plus
Certainly, procedural efficiencies are important, and many scheduling and EVV systems force caregivers to check in and check out in the presence of the patient and alert office staff when a caregiver arrives late or is a no-show. What we saw during our demo, however, we have not seen elsewhere. Compliance Plus automates the tedious task of rooting out EVV, billing, and payroll errors so efficiently, payment denials, aggregator rejections, and incorrect paychecks are virtually eliminated.
Mohammed confirmed what we saw in the demo. The file that includes hours, authorizations, patient demographics, and pre-arranged pay rates is prepared and perfected in advance. Then, the system uploads the same corrected file to the aggregator and to state and other payers. “If we need to fix hours or a bill, we do it before uploading to all entities,” he said. “We rarely get rejections from the aggregator or denials from payers.”
One of the requirements of payers and EVV aggregators is that all patient and caregiver names and other information must be in their respective databases in advance. Compliance Plus finds missing data and removes a bill from the file before it is uploaded, notifying the user with a red flag. Mohammed added, “We have to make sure all patient data is in system, but that is easy to do.”
Implementation and Training
In every home care agency, there is always a measure of trepidation among the staff when switching from familiar paper to automation. Aspen Home Care was no different when owner Ahmed Jara announced that he had accepted Hank’s invitation to join a beta test. Mohammed told us that his staff’s time from implementation to software expertise took a little less than three months. Compliance Plus customer relationship manager Sara Moore conducted online training of key office staff, a service that is included in Aspen’s monthly fee. Mohammed and a couple others trained the rest of the staff on the full system and then caregivers on the use of the app.
“After a short while, the new system became our normal workflow,” Mohammed commented. “The only speed bump is when they upload new features. We need to spend a little time learning them, but ultimately, the new features improve our workflow. Our caregivers pick up the app in about 30 minutes, including new hires.”
He added that his 200 caregivers like checking in and out on the app better than the legacy ANI system, which used the patient’s landline for automatic number identification. “English is a second language for some of our caregivers, and they sometimes had trouble with the ANI prompts spoken by the computerized voice,” he explained. “GPS verification is the best feature. If a caregiver checks in from too far away, we see their distance from the patient’s home on a map, and we gently ‘re-educated’ them and it does not happen again. In the past, they would sometimes get away with asking a family member to check in for them from the patient’s landline. Those days are gone.”
He also told us that Aspen does not insist on specific start times. What matters is that visit length matches authorized hours over a billing period. This is especially helpful for waiver and HCBS plans when the caregiver lives in the home. In those arrangements, checking in or out used to be easily forgotten. “I take care of her all day, how do I know when I start and stop?” The Compliance Plus app rings its cell phone loudly to remind visiting and live-in caregivers to check in and then to check out after the authorized number of hours have been reached.
Simplifying Complex Billing
Presently, Aspen exclusively serves Medicaid beneficiaries, though that can mean several managed care payers. With varying reimbursement rates from payers, combined with different caregiver hourly rates, getting a bill to match an authorization used to be a challenge for Office Manager Mohammed and his team.
In the case of an agency employed family caregiver, there are often days when the family member will spend one hour toileting and feeding, the next hour doing reimbursable homemaking chores, and the third hour running care-related errands. Not only might those tasks be paid at different rates, but they can, and often are, reimbursed by different payers.
Mohammed emphasized that the way Compliance Plus handles these situations saves considerable time and reduces payer and aggregator rejections. Like in a Venn diagram, every combination of patient, payer, task type, and caregiver creates a “patient profile.” The user created most profiles in advance, based on known payer rates, etc. Occasionally, a patient’s profile is unique, but a user can easily enter the specifics into the system manually. Once a profile is built, the system calculates all of the billing accurately without additional user supervision.
If a payer’s rate for a task changes, Mohammed or another office staffer makes the change one time for all affected patients. In that scenario where the live-in caregiver performs three different tasks in one day, he or she checks in and out only once, before the first task and after the last, and designates each task performed. Compliance Plus does the rest.
Hank Schwab told us that he is confident, after 100 successful beta customers, that Compliance Plus is ready for general release. At $10 to $12 per patient per month, he believes that supplementing word-of-mouth with a modest marketing effort will help him replace paper and strengthen the bottom line for many Medicaid and Personal Care agencies. Hank’s plan is to begin that effort as soon as he identifies an investor or two and hires a marketing director. “I already manage a team of coders and personally pay all the bills,” he laughed. “I’m ready for someone else to take on a few of my jobs.”
https://complianceplus.com/
*No, that is not a typo. We also enjoyed Mohammed Mohammed’s sense of humor. He tells people his parents were too cheap to give him a first name, so they just copied his last name.
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2025 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Tim Rowan | Aug 23, 2024 | Artificial Intelligence, Caring for the Caregiver, Clinical, CMS
by Tim Rowan, Editor Emeritus
O
ne just does not know whom to believe anymore. This week, we were sent three opinions of the pros and cons of Medicare Advantage programs. One says they reduce costs and improve patient satisfaction for rural residents. Another says rural hospitals are turning away MA customers at a growing rate. The third says MA customers utilize healthcare services at a lower rate than traditional Medicare beneficiaries. Let’s take a look at each opinion.
Better Medicare Alliance is a non-profit advocacy group that promotes Medicare Advantage. They describe themselves and the genesis of their recent report this way:
“Better Medicare Alliance engaged ATI Advisory to understand Medicare beneficiaries who live in rural areas and how they are served across Medicare Advantage and Fee-for-Service (FFS) Medicare. Understanding geographic differences in beneficiary experiences is important to both the Medicare Advantage and FFS Medicare program. This research can help policymakers and stakeholders identify opportunities to improve access to and quality of rural health care.”
That sounds good so far. Let’s look at their conclusions.
-
- 30 percent fewer MA client live in rural areas compared to cities and suburbs
- rural MA enrollees are more likely to be Black or LatinX but health needs are consistent across all rural demographics
- satisfaction is the same between rural MA clients and traditional Medicare beneficiaries, though MA enrollees use preventive services more and outpatient services less
- rural MA enrollees spend less in premiums and out of pocket costs than traditional Medicare beneficiaries
Rural Hospitals Tell a Different Story
Healthcare Uncovered, an online publication with a patient advocacy slant, describes BMA as “an active front group for the health insurance industry and perhaps the country’s greatest champion of Medicare Advantage plans.” and “with a well-stocked, industry-financed war chest to promote insurers’ premier product.”
Writing for Healthcare Uncovered, longtime healthcare journalist Trudy Lieberman added perspective to the BMA-sponsored report:
There was evidence last fall that Medicare Advantage was under attack when several hospitals announced they were reviewing their arrangements with Advantage plan sellers and were not accepting some or all plans. The CEO of the Brookings Hospital system in Brookings, South Dakota, told me, “The difference between original Medicare and Medicare Advantage is vast. Advantage plans pay less, don’t follow medical policy, coverage, billing, and payment rules and procedures, and they are always trying to figure out how to deny payment for services.”
In 2023, Becker’s Hospital Review began reporting on hospitals that were dropping some or all of their contracts with Advantage plans. The August 20, 2024 update indicates 18 more hospitals have or will drop MA plans this year.
Ms. Lieberman went on to report that MA plans frequently limit in-plan physicians. When they eliminate a physician in a rural community, patients often must travel miles to reach an approved doctor.
“Another damning report, this one issued by the Nebraska Rural Health Association, also revealed the pitfalls of joining an Advantage plan. The report warned that Nebraskans with Advantage plans ‘have created such a financial burden for rural residents’ that when they get sick, those with Medicare Advantage coverage ‘represent the largest growing segment of charity care for Nebraska’s rural hospitals.’ I’d bet few if any seniors are told they may end up on charity care if they choose an Advantage plan.”
A hospital in 23,000-resident North Platte, Nebraska has stopped accepting all MA patients. CEO Ivan Mitchell told Ms. Lieberman that transfers to nursing home and Home Health are denied 13 percent of the time. “Hospital stays are 40 percent longer for MA patients. They are stuck in the hospital two or three days waiting for approval to be transferred, and we need those beds for sicker patients.”
The Research Institute for Home Care awarded a grant to Tami M. Videon, PhD, and Robert J. Rosati, PhD, of the VNA Health Group, the honored Home Health not-for-profit in New Jersey. The researchers divided beneficiaries into three groups: Traditional Medicare, MA with a premium, and MA without a premium. Their findings resonated with the experiences of rural hospitals more than those of the MA advocacy group.
-
- Traditional Medicare (TM) beneficiaries were more likely to utilize outpatient, inpatient, and home health care services than beneficiaries in Medicare Advantage (MA) plans, regardless of whether the plan had a monthly premium or not.
- Beneficiaries who reported being in zero premium MA plans were substantially less likely to use dental, hearing, and vision services compared to other beneficiaries.
- Rates of utilization of hearing and dental services were relatively similar for beneficiaries reporting they were in MA plans with a premium and those enrolled in TM. Access to vision services was greatest among beneficiaries reporting being in MA plans with a premium.
In their research briefing, the researchers stated:
“Consistent with the literature, this study found beneficiaries enrolled in MA plans had lower utilization for services required to be covered by Medicare (outpatient visits, inpatient admission, and home health care use) than beneficiaries enrolled in TM. The observed lower rate of home health care utilization among MA beneficiaries may result from restrictions in inpatient care. However, prior research indicates when analyses are restricted to similar patient populations (a subset of diagnostic codes), MA beneficiaries are less likely to receive home health care than TM beneficiaries.”
We have often reported on the lawsuits that various federal departments have lodged against the largest health insurance companies for their Medicare Advantage practices. With their payments from the Medicare Trust Fund based on patient assessments, they have been caught exaggerating illnesses, adding chronic conditions that do not exist, and conducting periodic home visits to “update” their data on the health condition of their customers. These nurse visits to the home frequently “identify” serious health conditions that the person did not know they had, or in most cases did not have at all.
As a consequence of this practice, coupled with denying care that Traditional Medicare would have covered, the program has been determined by government audits to cost 119 percent of what Traditional Medicare costs.
Should Home Health follow the lead of so many rural hospitals and begin to Just Say No? Our guess is that this will be a prominent topic at this October’s NAHC Conference in Tampa.
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com Tim@RowanResources.com ©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only.
editor@therowanreport.com
by Tim Rowan | Jul 19, 2024 | Admin, Editorial, Medicare Advantage
by Tim Rowan, Editor Emeritus
UnitedHealth Making Home Health Visits
Payer or Competitor…that is the question. According to a report in the Wall Street Journal, and questioned by the insurance industry’s lobbying arm, AHIP, UnitedHealth Group has increased its revenue from the Medicare Trust Fund by $50 billion by “finding” additional health issues during home visits to its MA customers.
In a July 16 investor call, CEO Andrew Witty said UnitedHealth clinicians made more than 2.5 million home health visits to UnitedHealthcare MA members in 2023. Following these visits to more than 500,000 seniors, UnitedHealth upgraded over 300,000 of them to higher payment levels by uncovering health conditions the individual seniors did not know they had.
The WSJ investigation found that between 2018 and 2021, insurers received $50 billion for diagnoses they added to members’ charts. Many of these diagnoses were “questionable,” according to that investigation.
Though a UnitedHealth spokesperson called the analysis “inaccurate and biased,” former UnitedHealth employees told the Journal home visits are often used to add diagnoses. Clinicians say they use software during visits that offer suggestions as to what illnesses a patient might have.
CEO Witty maintained in the investor call that the practice is good for seniors. “UnitedHealth clinicians discovered more than 3 million gaps in care through home visits in 2023,” he reported, “and 75% of patients receive follow-up care in a clinic within 90 days of a home visit.”
He added that the United home visit program “helps patients live healthier lives and saves taxpayers money,” concluding. “…Medicare Advantage makes programs and results like this possible.”
The Journal concluded with the finding that few of these upgraded seniors are ever seen by a physician for their newly discovered health conditions.
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Tim Rowan | May 16, 2024 | Admin, Artificial Intelligence, CMS, Medicare Advantage, Regulatory
by Tim Rowan, Editor Emeritus
Lawsuits are beginning to pile up against insurance companies participating in the Medicare Advantage program. The complaint? The wrong way to use AI in healthcare is with faulty algorithms to approve or deny claims. While AI can be extremely helpful in streamlining administrative tasks — comparing physician notes with Home Health assessments and nursing notes or reading hospital discharge documents — it seems not to be any good at deciding whether to approve or deny care.
The Wrong Way to Use AI in Healthcare Example 1
The Minnesota case, November, 2023, UnitedHealth Group:
-
- An elderly couple’s doctor deemed extended care medically necessary
- UnitedHealth’s MA arm denied that care
- Following their deaths, the couple’s family sued UnitedHealth, alleging:
- Straight Medicare would have approved the extended care
- United uses an AI model developed by NaviHealth called nH Predict to make coverage decisions
- UnitedHealth Group acquired NaviHealth in 2020 and assigned it to its Optum division
- nH Predict is known to be so inaccurate, 90% of its denials are overturned when appealed to the ALJ level
- UnitedHealth Group announced in October, 2023 that its division that deploys nH Predict will longer use the NaviHealth brand name but will refer to that Optum division as “Home & Community Care.”
The family’s complaint stated, “The elderly are prematurely kicked out of care facilities nationwide or forced to deplete family savings to continue receiving necessary medical care, all because [UnitedHealth’s] AI model ‘disagrees’ with their real live doctors’ determinations.”
The Wrong Way to Use AI in Healthcare Example 2
The Class-Action case, December 2023, Humana:
-
- A lawsuit was filed on December 12, 2023 in the U.S, District Court for the Western District of Kentucky
- It was filed by the same Los Angeles law firm that filed the Minnesota case the previous month, Clarkson
- The suit notes that Louisville-based Humana also uses nH Predict from NaviHealth
- The plaintiffs claim, “Humana knows that the nH Predict AI Model predictions are highly inaccurate and are not based on patients’ medical needs but continues to use this system to deny patients’ coverage.”
- The suit says Medicare Advantage patients who are hospitalized for three days usually are eligible to spend as many as 100 days getting follow-up care in a nursing home, but that Humana customers are rarely allowed to stay as long as 14 days.
- A Humana representative said Humana their own employed physicians see AI recommendations but make final coverage decisions.
What Makes This Possible
According to experts we speak with, there are many ways to use data analytics. The insurance companies named in the lawsuits use predictive decision making. This way of analyzing data compares a patient to millions of others and deduces what treatment plan might be suitable for one patient, based on what was effective for most previous patients. Opponents of this method have called it “data supported guessing.”
A superior analysis method experts are coming to understand is prescriptive decision making. This is taking all of the available historical and current data surrounding a patient and making a clinical decision specifically designed to that patient’s age, gender, co-morbidities, doctor recommendations, and treatment records.
Until recently, predictive analysis was the preferred method because of its resource efficiency. Examining the data of every individual patient used to be prohibitively labor-intensive, requiring hours of reading hospital records, physician notes, and claims. Today, however, AI tools are able to do that work in seconds, making prescriptive analytics and customized plans of care possible.
Fix May Be in the Works
In a February 6, 2024 memo to all Medicare Advantage Organizations and Medicare-Medicaid Plans, CMS explained the difference between predictive and prescriptive analytics. The memo said these plans may not make coverage determinations based on aggregated data but must look at each individual:
“For Medicare basic benefits, MA organizations must make medical necessity determinations in accordance with all medical necessity determination requirements, outlined at § 422.101(c)1 ; based on the circumstances of each specific individual, including the patient’s medical history, physician recommendations, and clinical notes; and in line with all fully established Traditional Medicare coverage criteria.”
In response to a request for clarification, the CMS memo laid out its rule in specific language: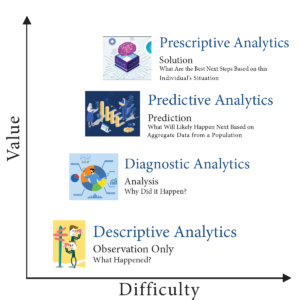
An algorithm or software tool can be used to assist MA plans in making coverage determinations, but it is the responsibility of the MA organization to ensure that the algorithm or artificial intelligence complies with all applicable rules for how coverage determinations by MA organizations are made. For example, compliance is required with all of the rules at § 422.101(c) for making a determination of medical necessity, including that the MA organization base the decision on the individual patient’s circumstances, so an algorithm that determines coverage based on a larger data set instead of the individual patient’s medical history, the physician’s recommendations, or clinical notes would not be compliant with § 422.101(c).
(emphasis added)
“Therefore, the algorithm or software tool should only be used to ensure fidelity with the posted internal coverage criteria which has been made public under § 422.101(b)(6)(ii).”
In further responses to questions in the same memo, CMS made it clear MA plans must make the same coverage decision original Medicare would make. The only allowable exception is that plans may use their own criteria when Medicare Parts A and B coverage criteria “are not fully established.”
Knowledge of this CMS directive may give Home Health agencies one more arrow in their quiver when going to battle with powerful, profit-oriented insurance companies over harmful, illogical AI algorithm decisions.
For information on the right way to use AI in healthcare, see our complimentary article in this week’s issue.
 Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report.homecaretechreport.com One copy may be printed for personal use: further reproduction by permission only. editor@homecaretechreport.com






