by Tim Rowan | Nov 13, 2025 | Artificial Intelligence, Clinical, New Tech
by Tim Rowan, Editor Emeritus
At this year’s annual meeting of The National Alliance for Care at Home, one could not attend a general or breakout session or walk an aisle in the exhibit hall without hearing about artificial intelligence. After 27 years covering Home Health, Home Care, and Hospice technology, I have seen buzzwords come and go. Declared game-changers have evolved from Windows to the iPad, to smartphones, to telehealth, to Big Data, to the Internet itself.
Interestingly enough, the “game” never changed. Patients/clients, nurses/CNAs, claims, payroll, and A/R have always, and will always, keep owners, administrators, and managers sprinting. AI will bring massive changes, but not to these constants.
AI is a Supplement, not a Replacement
There is much concern, and a plethora of articles, about how easily AI can be abused, even with the most noble intentions. We have detected serious concern about a movement to allow AI to make clinical decisions. We concur that this is inappropriate. Advising clinical decisions, providing background on previous patients with similar symptoms, or quickly accumulating data on the history of a chronic condition, can benefit our patients and clients in ways no other technology has been able to do. Making clinical decisions is different in both kind and degree.
This is why we were impressed with the focus on supplementing over replacing that we witnessed in New Orleans.
Ambient Listening for OASIS
When WellSky acquired Kinnser, everyone wondered whether the Home Health EMR would improve or merely be maintained for its customer base. Longtime friend of The Rowan Report, and WellSky and former Fazzi consultant Cindy Campbell, RN, convinced us with her uncharacteristic effusiveness to take another look at the latest WellSky feature.
During the OASIS visit, the nurse in the home logs into an app and places it between him/her and the patient. As the normal OASIS conversation takes place, the AI-enabled app not only hears but interprets every nuance of the chat. By the time the OASIS visit is over, the agency’s EMR has been fully populated. Every OASIS question has been answered, and every numerical rating field has been accurately completed.
Wisely, WellSky allows no AI OASIS assessment to be saved or signed without review by a human. This is going to become standard practice as AI evolves, or at least it should be, the WellSky rep told us. Machine assistance is far removed from machine perfection. Nevertheless, she asserted, few changes are required by the reviewer, usually a QA nurse.
In addition to streamlining the OASIS assessment visit, the new app gives voice reminders to each nurse of their daily and weekly schedule, and background information about each patient’s visit history, current condition, and goals.
Our AI tour did not end at the WellSky booth. We lost count of the number of smaller companies that were demonstrating the exact same AI-assisted OASIS assessment. It was as though some unknown force ordered, “OK, everyone. It’s 2025. Roll out your Home Health AI functions.”
Roger is the name of one of the more evolved such apps, from the aptly named Roger Healthcare. We had interviewed co-founder Yunus Ansari several months ago and were impressed by the product’s progress since then. Like WellSky and the others, Roger claims 15-minute OASIS visits, 5-minutes routine visit notes, 2-minutes EMR syncing, and larger per-nurse patient caseloads without additional work time.
Where Do We Go From Here?
Clearly, AI is not a fad. It has already permeated Amazon, Facebook, and most gas and electric vehicles. In Home Health, Home Care, and Hospice, it promises to accelerate research, education, paperwork, and revenue cycle management. Here is the red line in the sand. When used to enhance the efficiency and working knowledge of a nurse, CNA, or non-medical caregiver, it will go a long way toward helping in-home care to keep up with budget cuts, reimbursement reductions, inflation, and nurse/caregiver shortages.
When used to replace the clinical expertise of physicians, nurses, CNAs, and even personal care assistants, it smacks of HAL, the renegade computer of 2001: A Space Odyssey. What we need to do as AI infiltrates more and more aspects of our lives, is constantly remind ourselves that it is only a tool, not a master.
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2025 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | Aug 28, 2025 | CMS, OASIS, Regulatory
OASIS-E2 Instruments and Change Table draft are available from The Centers for Medicare & Medicaid Services (CMS). They are available for download here. The draft proposes an off-cycle implementation date of April 1, 2026
- Transportation listing changed from A1250 to A1255
- Hearing (B0200) and Vision (B1000) added to ROC
- Sex (A0810) replaces Gender (M0069)
- COVID vaccination up to date removed
- Language (A1110) added to ROC
- Minor changes to replace outdated item numbers with updated ones (ex: all instances of A1250 changed to A1255)
The Changes are effective April 1, 2026. However, the changes are not final pending approval from the Office of Management and Budget (OMB). Agencies are able to use the draft form for training purposes, but should look for the final form that includes the OMB control number and expiration date.
OASIS accuracy is linked to PDGM payments and quality outcomes. Prepare early for the off-cycle April 1, 2026 changes to ensure a smooth transition to E2 requirements and continued reporting accuracy.
Draft versions of the instruments are on the CMS website in a ZIP file. You can download the file here.
The PRA package, which includes four separate documents, is available for download here.
Submit comments to CMS about OASIS-E2 or any other item in the Home Health Prospective Payment System Rate Update for CY 2026 here and here.
by Kristin Rowan | Jan 23, 2025 | Admin, Clinical, Product Review
OASIS Assessment is a Time Suck
Regulatory requirements for home health quality assurance are designed to monitor and improve quality of care. QA focuses on ensuring that patients get safe, effective, compassionate care that meets their individual needs. QA also improves patient outcomes and reduces adverse events like ER visits and rehospitalizations. OASIS includes 79 standardized medical, nursing, and rehab data elements for a comprehensive assessment. Typical OASIS assessments take 1-2 hours to complete, depending on the patient’s complexity and the assessment type.
Artificial Intelligence in OASIS coding
The Rowan Report recently came across a tool that addresses the complexities of OASIS coding. We sat down with Zach Newman (CEO) and Dan Conger (Founder) at Enzo Health to learn more about their AI powered QA tool with customizable workflows.
Enzo Health is a documentation tool that automates workflows, acting as a co-pilot for your agency. Some of the workflows that Enzo Health supports include intake, OASIS, and QA reviews. Automating these processes can reduce errors and clawbacks, save your clinicians hours of paperwork, and offer cost savings to your agency.
With the Enzo health QA tool, users upload all documents related to an episode. This will include the referral, initial visit notes, patient information, medical history, and form 485. Enzo calls out any issues it finds in the documentation.
In Face-to-Face encounters, Enzo looks for dates, signatures from qualifying clinicians, a valid primary diagnosis, and other qualifying information.
For ICD-10 Coding, Enzo assesses primary and secondary diagnoses, and adds notes with links to where the information can be found in the uploaded documentation.
Enzo then provides functional limitations and improvements that can be made. Using a team of clinicians that are trained as home health coders, Enzo provides a proxy for internal teams. These coders review charts and finalize diagnosis coding and OASIS answers.
Qualification for an episode of care is required before anything else happens with a referral. Enzo’s intake automation tool reviews the referral package in advance of the initial F2F. Mirroring the agency’s internal intake process, Enzo determines whether the patient will be admitted to care, whether their insurance will cover the episode, and whether the patient’s psych history may impact the plan of care.
The Rowan Report has often stated, and will continue to stand by this fact, that there is no substitute for face-to-face care and the expertise of the nurses and clinicians in the home. We have also seen the advancement of artificial intelligence that provides assistance and guidance at the point-of-care that can be useful. Enzo health includes a chat tool that pulls evidence-based information to provide guidance, coding instructions, and other help to nurses.
QA Tool Integration with Scribe Tool
Enzo Health has developed a talk-to-text scribe tool that integrates directly with the QA tool. The use of both products together would likely save more time as well as reduce errors. The Rowan Report will provide a thorough product review of the scribe tool at a later date. Enzo Health charges a flat fee determined by volume and offers bundle pricing for using both the QA and Scribe tools.
Costs are increasing, the workforce shortage is ongoing, nurses are suffering from burnout, and employees are stretched about as thin as they can go. Any tool that alleviates paperwork, stress, unpaid work at home to finish documentation, and the need for additional back-office staff is worth looking into. Enzo differentiates its tool from other QA software with their team of clinicians trained in home health coding to review the documentation. This end-to-end tool boasts a 95% accuracy rate and do date has no clawbacks or ADRs.
In my conversation with Zach and Dan, their coding expertise and knowledge of the home health industry were evident. They are excited about the tools they are creating and passionate about helping agencies to provide patient care, a task they referred to as “very noble.” They continue to improve upon their software and conceive of innovative additions. If they continue as they started, Enzo Health will be one to watch.
by Tim Rowan | May 16, 2024 | Admin, Artificial Intelligence, Clinical, New Tech, Outcomes, Product Review, Vendor Watch
by Tim Rowan, Editor Emeritus
For better or worse, healthcare has begun the inevitable adoption of Artificial Intelligence. Before you consider adopting AI technology, know that there is a wrong way and a right way to use AI in healthcare. In a companion article this week, we describe the criticism insurance companies are getting for deploying AI in healthcare to harm patients. As a balance, here is a review of a product that we find to be using AI in healthcare to help both patients and Home Health Agencies.
The Problem
Home Health referral documents from physicians or hospitals can consist of more than 100 electronically transmitted pages. Some agencies report occasional packets exceeding 1,000 pages, often in a variety of data formats. Some are standard data formats, such as a face sheet, but most are unstructured, consisting of images or narrations, sometimes in paragraphs, sometimes in incomplete sentences. Worse, patient data interoperability can be limited by unstructured data.
More often than not, most of these pages are never read. Thoroughly interpreting that much data is nearly impossible for a human. Consequently, nurses too often approach an admission evaluation visit with an incomplete picture of a patient. The result can be gaps in care or treatment, inaccurate OASIS assessments, incomplete or poorly sequenced diagnosis codes, and improper care plans. These obstacles can impact both patient outcomes and agency revenue.
One Newly Available Solution for the Right Way to use AI in Healthcare
We recently attended a product demonstration and followed it up with updated descriptions to learn details about new product developments. Over the next three months, Select Data, in full disclosure one of our sponsors, will be introducing an AI-powered suite of products that has been designed over many years of development to support clinical, data driven decision-making. One by one, it addresses the problems described above.
The new system, SmartCare, empowers clinicians to harness previously hidden insights while reducing bias and cognitive overload. It enables them to steer their decisions with enhanced precision while maintaining their pivotal role in patient care, eliminating one of the common reasons many Home Health administrators hesitate to invite AI into agency processes. It does, however, make the care team’s job easier and facilitates better decision-making.
- AI can read those 100 to 1,000 page referral documents in minutes, where a human may require days.

- SmartCare uses AI to synthesize relevant medical history to provide a care snapshot highlighting the key diagnosis, focus and considerations for care, and recommended OASIS clinical discipline. It highlights any areas for clarification needed from physician or admitting nurse.
- Clinicians can search and index specific words in unstructured data, such as narratives, to instantly identify any detail of a patient’s condition in an easy-to-read interface. Nurses approach the initial OASIS visit armed with all of a referring clinician’s relevant care findings.
- Recommendations for diagnostic codes strictly follow Medicare PDGM guidelines.
Suite of Tools
1 – RISE stand for Rapid Intake Summary & Evaluation. This component of the suite summarizes all clinical data from referral sources and your EHR. It compiles this data to provide clinically relevant diagnoses, focus of care, and recommendations for skilled disciplines. This is the part of the tool that reads referral documents and supports informed decision-making. The advantages we detected go a bit beyond the technical.
When clinicians, reviewers, coders, and office staff all have access to the same patient information, it would seem that communication among disciplines would improve and that care coordination would be enhanced. It also seems logical that continued experiences of advanced access to previously hard-to-find physician comments would gradually break through the AI fear barrier reported by so many clinicians and other professionals. Select Data will provide us with actual client experiences to verify our assumptions once they have been compiled.
2 – ACE, or Admission Clinical Evaluation is SmartCare’s clinical support summary tool. It deploys AI to understand accepted OASIS assessment criteria. It then uses this knowledge to extract assessment and narrative data from nursing and therapy evaluations. With streamlined, pertinent data at the point of care, the entire care team has the same patient data. Having the same patient data enables more informed decision-making.
ACE links all patient data back to its source assessment. Doubt about the AI’s credibility should gradually diminish, even among the most AI-resistant users. Every analysis and recommendation is explained in clear language so that clinicians are likely to understand the rationale behind them. The goal is to replace every “I’m not going to let a machine tell me what to do” with “I’ll take this information into consideration with my human insights.”
Pricing
We are honoring Select Data’s request to allow them to build personalized price quotes to every prospective client. They will be represented at several state and national conferences this year. Alternatively, interested HHA representatives can contact EVP Ted Schulte at Ted.Schulte@SelectData.com
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report.homecaretechreport.com One copy may be printed for personal use: further reproduction by permission only. editor@homecaretechreport.com
by Tim Rowan | May 16, 2024 | Admin, Artificial Intelligence, CMS, Medicare Advantage, Regulatory
by Tim Rowan, Editor Emeritus
Lawsuits are beginning to pile up against insurance companies participating in the Medicare Advantage program. The complaint? The wrong way to use AI in healthcare is with faulty algorithms to approve or deny claims. While AI can be extremely helpful in streamlining administrative tasks — comparing physician notes with Home Health assessments and nursing notes or reading hospital discharge documents — it seems not to be any good at deciding whether to approve or deny care.
The Wrong Way to Use AI in Healthcare Example 1
The Minnesota case, November, 2023, UnitedHealth Group:
-
- An elderly couple’s doctor deemed extended care medically necessary
- UnitedHealth’s MA arm denied that care
- Following their deaths, the couple’s family sued UnitedHealth, alleging:
- Straight Medicare would have approved the extended care
- United uses an AI model developed by NaviHealth called nH Predict to make coverage decisions
- UnitedHealth Group acquired NaviHealth in 2020 and assigned it to its Optum division
- nH Predict is known to be so inaccurate, 90% of its denials are overturned when appealed to the ALJ level
- UnitedHealth Group announced in October, 2023 that its division that deploys nH Predict will longer use the NaviHealth brand name but will refer to that Optum division as “Home & Community Care.”
The family’s complaint stated, “The elderly are prematurely kicked out of care facilities nationwide or forced to deplete family savings to continue receiving necessary medical care, all because [UnitedHealth’s] AI model ‘disagrees’ with their real live doctors’ determinations.”
The Wrong Way to Use AI in Healthcare Example 2
The Class-Action case, December 2023, Humana:
-
- A lawsuit was filed on December 12, 2023 in the U.S, District Court for the Western District of Kentucky
- It was filed by the same Los Angeles law firm that filed the Minnesota case the previous month, Clarkson
- The suit notes that Louisville-based Humana also uses nH Predict from NaviHealth
- The plaintiffs claim, “Humana knows that the nH Predict AI Model predictions are highly inaccurate and are not based on patients’ medical needs but continues to use this system to deny patients’ coverage.”
- The suit says Medicare Advantage patients who are hospitalized for three days usually are eligible to spend as many as 100 days getting follow-up care in a nursing home, but that Humana customers are rarely allowed to stay as long as 14 days.
- A Humana representative said Humana their own employed physicians see AI recommendations but make final coverage decisions.
What Makes This Possible
According to experts we speak with, there are many ways to use data analytics. The insurance companies named in the lawsuits use predictive decision making. This way of analyzing data compares a patient to millions of others and deduces what treatment plan might be suitable for one patient, based on what was effective for most previous patients. Opponents of this method have called it “data supported guessing.”
A superior analysis method experts are coming to understand is prescriptive decision making. This is taking all of the available historical and current data surrounding a patient and making a clinical decision specifically designed to that patient’s age, gender, co-morbidities, doctor recommendations, and treatment records.
Until recently, predictive analysis was the preferred method because of its resource efficiency. Examining the data of every individual patient used to be prohibitively labor-intensive, requiring hours of reading hospital records, physician notes, and claims. Today, however, AI tools are able to do that work in seconds, making prescriptive analytics and customized plans of care possible.
Fix May Be in the Works
In a February 6, 2024 memo to all Medicare Advantage Organizations and Medicare-Medicaid Plans, CMS explained the difference between predictive and prescriptive analytics. The memo said these plans may not make coverage determinations based on aggregated data but must look at each individual:
“For Medicare basic benefits, MA organizations must make medical necessity determinations in accordance with all medical necessity determination requirements, outlined at § 422.101(c)1 ; based on the circumstances of each specific individual, including the patient’s medical history, physician recommendations, and clinical notes; and in line with all fully established Traditional Medicare coverage criteria.”
In response to a request for clarification, the CMS memo laid out its rule in specific language: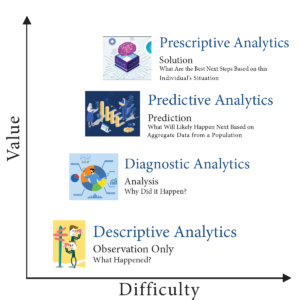
An algorithm or software tool can be used to assist MA plans in making coverage determinations, but it is the responsibility of the MA organization to ensure that the algorithm or artificial intelligence complies with all applicable rules for how coverage determinations by MA organizations are made. For example, compliance is required with all of the rules at § 422.101(c) for making a determination of medical necessity, including that the MA organization base the decision on the individual patient’s circumstances, so an algorithm that determines coverage based on a larger data set instead of the individual patient’s medical history, the physician’s recommendations, or clinical notes would not be compliant with § 422.101(c).
(emphasis added)
“Therefore, the algorithm or software tool should only be used to ensure fidelity with the posted internal coverage criteria which has been made public under § 422.101(b)(6)(ii).”
In further responses to questions in the same memo, CMS made it clear MA plans must make the same coverage decision original Medicare would make. The only allowable exception is that plans may use their own criteria when Medicare Parts A and B coverage criteria “are not fully established.”
Knowledge of this CMS directive may give Home Health agencies one more arrow in their quiver when going to battle with powerful, profit-oriented insurance companies over harmful, illogical AI algorithm decisions.
For information on the right way to use AI in healthcare, see our complimentary article in this week’s issue.
 Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report.homecaretechreport.com One copy may be printed for personal use: further reproduction by permission only. editor@homecaretechreport.com
by Rowan Report | Oct 11, 2023 | CMS, Medicare Advantage, Regulatory
NOW AVAILABLE IN iQIES – Preview Reports and Star Rating Preview Reports for the January 2024 Refresh
CMS just published updated measure for Home Health Outcome Information Set (Oasis) and all HH QRP claims-based measures. These updated measures are no based on the standard number of quarter.
For additional information, please see the HH Quality Reporting Training webpage and the Home Health Data Submission Deadlines webpage.
©2023 by Rowan Consulting Associates, Inc., Colorado Springs, CO. This article originally appeared in Home Care Technology: The Rowan Report. Click here to subscribe. It may be freely reproduced provided this copyright statement remains intact. editor@homecaretechreport.com







