by Kristin Rowan | Jun 27, 2024 | CMS, Regulatory
CMS Proposed Rule for 2025
Citing “budget neutrality adjustments”, the Centers for Medicare & Medicaid Services (CMS) June 26 issued its proposed rule for 2025 for the home health prospective payment system. Here are the highlights:
- Overall net reduction in home health payments by $280 million dollars
- Market basket update of 3.0%
- Productivity adjustment of -0.5%
- Base payment rate reduction of 4.067% due to PDGM
- Update fixed dollar loss for outlier payments
- Update LUPA thresholds, functional impairment levels, and comorbidity adjustment subgroups
We did the math. This is an overall reduction in payment by 3.6%. This come after multiple years of similar adjustments that reduced the overall payment rates.
Included in the proposal is an additional adjustment to the fixed-dollar loss amount for high-cost outliers. This will reduce payments another 0.6%.
As we focus primarily on the payment reductions, CMS is looking at additional data. CMS provides a detailed account of the requirements for behavior assumptions and actual changes, as outlined in earlier rules. Using CY 2023 claims, and the methodology from the CY 2023 final rule, CMS believes they paid more under the PDGM system than they would have under the old system, leading to the deduction in base payment rate.
HHA Conditions of Participation
In addition to the payment cuts, CMS is also proposing an update to the Conditions of Participation. This new standard would require HHAs to develop, apply, and maintain a policy for accepting new patients into service.
According to the proposal, CMS is not moving to add or modify any quality measures from the Quality Reporting Program. They do, however, propose to modify some patient assessment items related to health-related social needs. This would require HHAs to collect and report data related to living situation, food, and utilities. This proposed modification would be implemented beginning with the calendar year 2027 QRP.
Also included in the CY 2025 proposal is a revision to the infection prevention and control requirements for long-term care facilities. The revision calls for an extension on reporting some of the Covid-19 data elements to the Centers for Disease Control and Prevention. It also requires influenza and RSV reporting beginning January 1, 2025.
CMS also used data from OASIS-D and OASIS-E, making adjustments for missing and altered data from the two different information sets. The proposed rule includes a new methodology to address the issue of varying data sets from OASIS-D to OASIS-E.
LUPA add-ons are meant to establish equitable compensation for all home health services. CMS is proposing an occupational therapy (OT) specific LUPA add-on factor, rather than continuing to use the PT add-on factor for OT.
Payment groups under the PDGM model use an associated case-mix weight and LUPA threshold, specific to each of the 432 payment groups. CMS is proposing a recalibration of the case-mix weights, including funtional levels and comorbidity adjustment subgroups.
Request for Information: CMS is seeking feedback on Future Performance Measure Concepts for the expanded HHVBP Model. New proposed measure include care activities like bathing and dressing, which are not currently included in the function measures. Additional potential measures include family caregiver status and claims-based falls with major injuries.
The American Hospital Association has expressed “serious concerns” about the payment rate adjustments in the proposed rule. “We urge the agency to adequately resource HH providers as they are a critical part of the care continuum,” AHA wrote. “We are particularly concerned about the substantial size of the agency’s proposed budget neutrality adjustment, a cut of 5.653%, and again call on CMS to withdraw it.” The AHA has asked CMS to revise its accounting methodology to more accurately account for changes in the payment system and care delivery due to PDGM.
President of the National Association for Home Care and Hospice (NAHC), Bill Dombi, today released a statement:
“The 2025 proposed version of Medicare home health payment rates shows the ongoing and predictable rate reductions impacting home health agencies since the beginning of the new payment model in 2020. That decline is solely due to a fatally flawed budget neutrality methodology that CMS employed to arrive at the rate adjustments,” stated NAHC President William A. Dombi.
“While this means that Medicare spending on home health services will continue to decline as costs continue rise, the more important element is that care access and utilization continues to decline at significant levels. When Congress set Medicare payment reform in motion starting in 2020, it was not planned or even expected that the outcome would be that nearly 500,000 Medicare beneficiaries would be able to access care or that those who could find care would get fewer services,” he added.
“Congress must step in immediately to put an end to this dismantling of the Medicare home health benefit. The value of home health services is not only undeniable; it has been proven by CMS in its analysis and expansion of the highly successful Home Health Value Purchasing demonstration project. We call on Congress to correct what CMS has done and prevent the growing harm to the millions of highly vulnerable home health patients that depend and will depend in the future on this essential Medicare benefit. Fortunately, longstanding advocates for home health care, Senator Debbie Stabenow (D-MI) and Senator Susan Collins (R-ME) have introduced S. 2137 to eliminate the rate cuts. We urge the Congress to support this legislation and enact it into law before the end of the year. The 2025 rate cuts must not take effect” Dombi added.
CMS has issued a fact sheet with more details on their assumptions and calculations. You can access the fact sheet here. The proposed rule can be downloaded here.
CMS will accept comments on the proposed rule through August 26th.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | Jun 13, 2024 | Clinical
by Kristin Rowan, Editor
The Home Health Value-Based Purchasing (HHVBP) Model began in 2016 as part of the Home Health Prospective Payment System (HH PPS) final rule. The original model aimed to:
- Incentivize better quality and more efficient care
- Study potential quality and efficiency measures
- Enhance the public reporting process
The original model had an average 4.6 percent improvement in Total Performance Scores (TPS). The model also saved Medicare $141 million annually, on average. There were no adverse risks with these savings.
Additionally, the model reduced the number of unplanned hospitalizations and stays at Skilled Nursing Facilities (SNF). This provided additional savings from lower inpatient and SNF spending.
The HHVBP model expanded in 2022. The model includes HHAs in all 50 states, D.C., and the U.S. territories. The model adjusts Medicare payments from the fee-for-service (FFS) model. Quality measures in a Performance Year impact adjustments in the Payment Year. These adjustments range from -5% to 5% and are based on quality measures relative to peer performance. HHA peers are pre-assigned cohorts with HHAs of similar size.
The expanded HHVBP model uses data from the Home Health Quality Reporting Program (HH QRP), Medicare claims, and HHCAHPS surveys. The expanded model does not require any additional data at this time.
Additional information on the quality measures, cohorts, guides, and recordings from CMS can be found here.
We will continue to follow this story and provide updates on the new expanded model as they come in.
# # #
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | May 30, 2024 | Admin, Advocacy, CMS, Regulatory
by Kristin Rowan, Editor
NAHC President Bill Dombi announced at last week’s CAHSAH annual meeting and expo that he would end his tenure at NAHC and retire at the end of 2024. We reached had an interview with Dombi on Thursday, May 23rd. He said he was not prepared to speak yet about his upcoming retirement, but we should hear more about that soon.
In the meantime, he provided additional details from his session at CAHSAH. We also discussed updates on the lawsuit against CMS and the status of the merger between NAHC and NHPCO. Tim’s article from last week talks about Dombi’s progress with Senator Wyland.
Ongoing Litigation
When we last spoke with Bill, he told us about the lawsuits filed against CMS. The suit claims that the budget-neutral calculations were based on faulty data and outdated software. These calculations determined the reimbursement rate reductions. Dombi explained the process for those lawsuits.
“The first round of the battle is around whether the court has the power to hear the case either at all or at that point in time. The courts are littered with litigation that have been dismissed on jurisdictional grounds,” Dombi offered. The court dismissed the lawsuit and the case is now closed. The Department of Justice (DoJ) attacked jurisdiction to get the case dismissed. Most concerning, according to Dombi, was the DoJ’s question of whether the statute passed by Congress precluded any litigation. If the courts had found in their favor, they would have dismissed the lawsuit no further suits could be filed. Luckily, that argument didn’t hold. The second attack was whether NAHC had expedited administrative review, which is the argument that caused the dismissal. Now, they have to establish that it would be futile to get CMS to agree to expedited judicial review.
Next Steps
In light of the dismissal, NAHC had to decide whether to appeal the ruling, exhaust the expedited review step with CMS, or both. Ultimately, they decided not to appeal and is pursing the review with CMS. This process could take up to 6 months, according to Dombi. Although they are pursuing the review, CMS has already stated that their final position is that the budget neutrality has been calculated within the law. Dombi feels the review is futile because CMS is not going to change their position. Now, they just have to prove the futility.
Two-Step Approach
Advocacy from NAHC, NHPCO, and other individuals and organizations was always intended to be a two-pronged effort: Litigation and Congress. The two do not interfere with each other. Even though the court dismissed the litigation suit in favor of judicial review, the approach in Congress continues. Of Senator Wyland, Dombi said, “A year ago at this time, his view was that home health agencies needed no relief. Now, he’s indicated a willingness to find a way to help home health agencies and recognizes that the cuts have been harmful to home health agencies and others that provide care.” According to Dombi, it was the personal stories and individual provider information that was crucial in swaying Wyland. The organizations continue to meet with other members of Congress to persuade them in the same way.
Dombi Provides Merger Update
Last year, NAHC and NHPCO announced they would join forces and merge into a new, as yet to be named, organization. That merger is still moving forward, but there are a lot of odds and ends to tie up. Dombi told us, “Nothing is final, final, but I don’t see anything but tailwinds moving forward.” The two organizations are still hoping for a July 1, 2024 launch of the organization. There is an active, open search for a new CEO to actively run both organizations as one. According to Dombi, no one has been slated for that position yet, so they may end up launching before there is a CEO in place.
The two organizations have already started integrating. They have lobbied together and they have worked on policy together. Additionally, they are integrating the association management system and building a website. “We feel confident enough that it’s going to reach the finish line that we’re investing time and money in these elements,” Dombi said. The two organizations can continue to operate together without a CEO, but there are a lot of decisions that need to be made that won’t be made until after there is a CEO.
After the Merger
Once the merger is complete and the two organizations operate under a new name with a new CEO, Dombi and his counterpart Bill Marcantonio of NHPCO will stay on for some time. Dombi will take the title President Emeritus and Council to the organization and Marcantonio will become the Chief Integration Officer. The new name of the organization has not been announced. Dombi says a lot of things are tied together, from an action standpoint, and it’s better to announce all of those details together along with the new name.
Reflections From Bill Dombi
When asked what was next for him after the merger is completed and he moves to retirement, Dombi reflected on his career:
“I’m proud of what I’ve accomplished in my life, but I’m more proud of what the people I work with I have accomplished. It’s not the first time we’ve tried to merge the two organizations, but this time, we had all the right ingredients and I’m proud of that. I live with the confidence that my constituency is up to the challenge. Every time they get kicked back, they’re right back at it.
To see where we are today compared to the 70s, we are so many light years ahead of where we were then. I mean, we’re talking about a hospital level of care at home. That was part of the dream. The fore-runners of healthcare at home truly believed those things were possible. The problems that caused the workforce shortage are multi-faceted, so the solutions are multi-pronged.”
We will continue following the story of both the lawsuits and the merger and update you as soon as there is more information.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or
www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only.
editor@therowanreport.com
by Tim Rowan | May 22, 2024 | Admin, CMS, Regulatory
by Tim Rowan, Editor Emeritus
For the last time, NAHC President Bill Dombi is spending another Spring on airplanes. It is state association meeting season, and the Bill Dombi Spring Tour has been bringing his regular Capitol Hill update from coast to coast, this time adding the announcement that he will retire at the end of the year.
After 40 years with NAHC, the lengthy standing ovation Californians gave him at the end of his Tuesday speech was well-deserved.
Advocacy and Change
Bill’s core message has not changed, though the details of his ongoing battle to force CMS to take HHAs and Hospices more seriously has its 2024-2025 nuances. “Letting Congress know that you are an important healthcare sector, and clearly the most popular sector, is not NAHC’s job alone. Every one of you has power. Use it. Make your voices heard.”
Meetings with the Senate Finance Committee
To illustrate the point, he related a story about his recent visit to Portland to meet with the Chair of the Senate Finance Committee, Ron Wyland (D-OR).
“Senator Wyden has been one of the major roadblocks to Medicare agencies getting fair payment rates. I went to see him with a group of agency owners and workers to describe the hardships the current and planned pay rate cuts will impose, and to explain the exact problems with the dumb formula CMS is using to calculate those pay rates.
“The Senator said, ‘But MedPAC says you make too much money and rates should be cut. Were they wrong? Or has something changed?’
Reaching Agreement…Almost
“Both, the group and I harmonized. One by one, each agency representative told him about the growing demand of an aging population, the difficulty hiring staff with the salaries our low pay rates allow them to pay, and a full litany of all the problems with Medicare Advantage.
“By the end of our meeting, we hadn’t turned him 180 degrees, but I could see he was beginning to turn.”Later, Dombi added, he met with Senator Debbie Stabenow (D-MI), who is not only a member of the same Finance Committee but the fourth in line in the Senate pecking order. She offered to have a conversation with her colleague, and that turned Senator Wyden the rest of the way toward changing his position 180 degrees.
You Can Make a Difference
“If you think you as an individual owner have no power in Sacramento, Congress, or the White House,” Dombi concluded, “think again.”
See sidebar for the complete list of Finance Committee members. Everyone has power, but if you are a voter in one of their states, you have an even more powerful voice.
The Bill Dombi Spring Tour will continue throughout the year until his retirement. Join Dombi at the 2024 Financial Management Conference & Expo in Las Vegas, July 21-23 and at the 2024 Home Care and Hospice Conference and Expo in Tampa, October 20-22.
Senator Ron Wyland (D-OR)
SENATE FINANCE COMMITTEE MEMBERS
Chair: Ron Wyland (D-OR)
Ranking Member: Mike Crapo (R-ID)
Debbie Stabenow (D-MI)
Chuck Grassley (R-IA)
Maria Cantwell (D-WA)
John Cornyn (R-TX)
Robert Menendez (D-NJ)
John Thune (R-SD)
Thomas Carper (D-DE)D-
Tim Scott (R-SC)
Benjamin Cardin (D-MD)
Bill Cassidy (R-LA)
Sherrod Brown (D-OH)
James Lankford (R-OK)
Michael Bennet (D-CO)
Steve Daines (R-MT)
Bob Casey (D-PA)
Todd Young (R-IN)
Mark Warner (D-VA)
John Barrasso (R-WY)
Sheldon Whitehouse (D-RI)
Ron Johnson (R-WI)
Maggie Hassan (D-NH)
Thom Tillis (R-NC)
Catherine Cortez Masto (D-NV)
Marsha Blackburn (R-TN)
Elizabeth Warren (D-MA)
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com
Tim@RowanResources.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report.homecaretechreport.com One copy may be printed for personal use: further reproduction by permission only. editor@homecaretechreport.com
by Kristin Rowan | Apr 26, 2024 | CMS, Recruitment & Retention, Regulatory
by Kristin Rowan, Editor
The Centers for Medicare and Medicaid Services (CMS) has finalized the “Ensuring Access to Medicaid Services” rule, more commonly known as the 80/20 rule. The 80/20 finalized rule requires at least 80% of Medicaid payments for home care services goes to caregiver wages. No more than 20% can be spent on administrative or other overhead costs. The White House, citing a study by The Commonwealth Fund, says that higher wages for caregivers will reduce turnover. Facing massive workforce shortages, home health, hospice, and supportive care at home agencies have been struggling to recruit and retain an adequate number of caregivers. The higher wage will also increase the quality of care, according to the study.
Prior to the 80/20 rule, there was no law or rule requiring home care agencies to report how they were spending money from federal medical payments. The rule includes requirements for states to create advisory groups to consult on rates and compensation. This changes the current Medical Care Advisory Committee regulations by increasing the percent of beneficiaries on the committee from 10% to 25% over the next two year. The Home Care Association of America (HCAOA) and the National Association for Home Care & Hospice (NAHC) argued that the rule adds administrative requirements to home care agencies while simultaneously reducing the resources available to fund them. NAHC President Bill Dombi said, “We all agree that more needs to be done to support the direct care workforce; however, this policy will make things worse, not better.” NAHC suggests the policy will force some agencies to close and others will leave the Medicaid program altogether, causing patients to have even more problems accessing care.
From the text of the final rule, CMS acknowledges additional comments that the minimum direct payment to caregivers in this rule will create hardships for some agencies. Across the country, there are substantial differences among waiver programs for HCBS that are not accounted for in the rule. There is some flexibility built into the rule to account for these factors, according to CMS. Some of the flexibilities include:
- Excluding some costs from the calculation
- Including clinical supervisors in the calculation
- Allowing states to set a different minimum for small providers
- Allowing states to develop their own criteria to qualify as a small provider
- Allowing states to develop criteria to exempt some providers from the rule
- Exemption from the minimum payment rule for all Indian Health Service and Tribal health programs
The final rule also changes the timeline for complying with the rule from four years after the date of publication to six.
Other comments included the need to address various reasons for the workforce shortage. In addition to low wages, commenters cited the social valuation of direct care work, lack of governmental support for some workforce pipelines, and immigration policies as deterrents to recruitment. One suggested that CMS start looking at creative strategies for developing an atypical workforce.
There were several submitted comments stating the either HHS or CMS or both does not have the authority under the Affordable Care Act to make specific requirements for minimum payments, but only to ensure that each State is assessing payment regulations and ensuring payments are economical, efficient, and ensure quality of care. A specific section of the Affordable Care Act, section 2402(a)(1) requires the Secretary of the Department of Health and Human Services (HHS) to ensure states implement service systems to allocate resources. The provision does not give HHS the authority to dictate the terms of those service systems, only to ensure the states develop those systems. Not surprisingly, CMS disagreed with those comments.
Many people questioned the 80% as being unrealistic, too high, and not based on quality data. CMS cited data from several states, who have pass-through requirements of 80-95% for all rate increases. This is not a minimum payment from all Medicaid payments, only a requirement for a minimum pass-through to direct care workers of increases in rates. Two states, Minnesota and Illinois, currently have minimum payment requirements set at 72% and 77%, respectively. CMS used these two states as justification for the 80% rule, acknowledging that it is higher than both states while also acknowledging that they did not perform a state-by-state study of the impact the 80% rule will have. CMS states the rate was set higher than those states to “encourage further steps towards improving compensation for workers.” CMS believes that requiring HCB agencies to pay their direct care workers a higher percentage of Medicaid rates than any state currently does will somehow make those agencies want to voluntarily pay even more.
The 80/20 Rule and Technology
Technological advances in telehealth, remote patient monitoring, revenue cycle management, scheduling, employee benefits, assistive technology, EVVs, EMRs, CRMs, and other software solutions can and will lower overhead costs and increase efficiency in your agency. Paperwork automation can reduce the time spent on documentation by a significant percentage. Revenue Cycle Management software can reduce claim denials and decrease reimbursement payment cycles so you can get your money faster. They can also reduce the number of unpaid claims. Employee benefit and training software can reduce responsibilities for HR teams, lessen the requirements for clinical supervisors, and cut training time in half, getting your newly recruited caregivers out in the field faster. Scheduling and onboarding software can increase your intake capabilities. The advances in generative AI allow you to create robust reports almost instantly so you can see your agency’s strengths and weaknesses and create plans for improvement.
Some of these costs will be excluded from the calculations for the 80% rule. Now is the time to invest in technology for your agency. Not only will your agency be more efficient and more effective, but you will be able to care for more patients with the same staff you have now, and the software solutions are as close to cost-neutral as they will ever be. We have a list of technology solutions that we’ve recently discovered and will be writing about in the next few weeks. If you are in immediate need of a software solution, contact us directly for a consultation.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | Apr 26, 2024 | CMS, Medicare Advantage, Regulatory
By Beth Noyce, RN, BSJMC, BCHH-C, COQS
CHAP-certified home health & hospice consultant
This is part 3 of the 3 in the series, outlining the discussions and implications in adopting new outcome and process measures for Hospice care. The final segment addresses future process and outcome measures that the board discussed, but did not yet implement. Read Part 1 on Outcome Measures and Part 2 on Process Measures.
The TEP discussed potential future process and outcome measure concepts that Abt Associates presented to the panel as well.
The process measures included:
- Education for Medication Management
- Wound Management Addressed in Plan of Care
- Transfer of Health Information to Subsequent Provider
- Transfer of Health Information to Patient/Family Caregiver
Hope-based outcome measures were:
- Patient Preferences Followed throughout Hospice Stay
- Hospitalization of Persons with Do-Not-Hospitalize Order
Developing education for medication management as a process measure was a popular concept, and the top priority of the recommended measures with the TEP as they “broadly agreed that CMS should develop this measure,” the report says, citing “a significant need for training in medication management for patients and their caregivers.” They recommended that the measure weigh more heavily when care is provided in a home setting than in a facility setting because hospices are unable to control facility training and hiring practices. One panelist commented that including the phrase “during today’s visit” in the measure is important.
Whether CMS should further develop the process measure addressing wound management in the plan of care was less straight-forward, as panelists provided varied feedback. They generally agreed that this measure is important, as having a record of wound management addressed in the plan of care can hold the staff accountable for treating the wounds. But some members recommended measuring wound management with outcome measures rather than process measures. One panelist cited potential problems from patients’ deterioration over time and another noted that the time frame of this measure is important, and encouraged recording the process of getting care in place once a wound is identified. The panel agreed CMS should carefully define the measure’s specifications.
Because standard practice for most agencies is, when a patient is discharged live, to transfer health information to the subsequent provider and to the patient and family or caregiver, TEP members expressed that the two measures were likely to “top out,” meaning they would almost always be marked “Yes,” making them of no value in differentiating between hospice providers. The group generally discouraged developing these process measures.
The group strongly rejected any merit in developing two outcome measures concerning Patient Preferences Followed Throughout Hospice Stay and Hospitalization of Persons with Do-Not-
Hospitalize Order. The report says “Multiple TEP members described situations in which patients who had preferred not to be hospitalized changed their minds when a crisis occurred. Patients’ preferences and unexpected crises are usually out of the hospice’s control. Although it is still important for hospices to ask patients about their preferences as part of patient-centered care, the TEP did not believe these two items would be practical measures of a hospice’s care quality.”
Dr. McNally expects that Abt. Associates will apply the HQEP TEP’s suggestions to the HOPE tool.
“Oh yeah, they did it,” he says. “Abt would come to a specific meeting with information, data, suggestions, and specific information about how these things would be measured. We’d give feedback. Then they’d come back to the next meeting having incorporated our suggestions,” he explains. “All of us felt very much heard and responded to. It didn’t feel in the least bit perfunctory.”
Whatever specific measures are eventually included in the HOPE tool, Lund Person sees value in its implementation. “Hospice providers have had a woeful lack of outcome measures for hospice patients, which has made the evaluation of quality hospice care based only on process measures and the family’s evaluation of hospice care in the CAHPS® Hospice Survey, she explains. “Implementing HOPE will begin to identify outcome measures that can be compared between providers.”
Lund Person warns of potential challenges as well. “The selection of risk adjustment and stratification must be carefully done to minimize bias and maximize effectiveness of measures,” she says. “In addition, hospice providers have been awaiting the release of the HOPE tool with significant anxiety about content and administrative burden.”
Dr. McNally is confident the HOPE tool will be a healthy change for hospices.
“A lot of my role as a medical director and hospice physician is supporting our nurses,” he says. “They do 95% of the work. I really would like to see this not be burdensome for our hospice nurses. I’m looking forward to seeing what the [HOPE tool] beta testing translates to in our own hospice world.” He added “What I would hope to see is that the tool feels user-friendly to the hospice team, the people who have to use it, and that it also provides useful information to patients and families.”
NAHC’s Wehri says that standardizing processes through the HOPE tool is the key foundational element for the hospice industry. “High quality care is driven by reducing variance through standardized processes, Wehri writes. “Also, CMS will have a better idea of how the type of population a hospice serves impacts some of the clinical care.” This small glimpse into hospice variances that CMS does not currently have could be very helpful in future policy and payment decisions, according to Wehri. “What CMS finds in terms of differences between hospices and their care for patients may be a bit of a surprise to CMS,” she says. “I hope they are pleasantly surprised with the overall quality of care that is revealed.”
# # #
 Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.
Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | Apr 18, 2024 | Clinical, CMS, Regulatory
by Beth Noyce, RN, BSJMC, HCS-C, BCHH-C, COQS
CHAP-certified home health & hospice consultant
Process Measures
The outcome measures being considered look at effectiveness of hospice clinical efforts to decrease pain and other symptoms. The process measures paired with them focus on the hospice’s follow up with the patient after moderate or severe symptoms are found during assessment.
Exhibit 6 (below) shows the numerator and denominator for these.
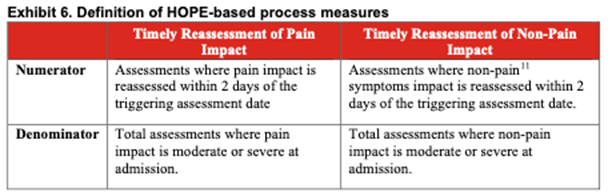
TEP members determined that these two process measures have high face validity. This means the measure items clearly state, or “look like” they will measure what CMS intends them to measure. This allows consumers to see what hospices are assessing and treating. It can also help hospices track how well they are reducing or treating patients’ symptoms.
Katie Wehri, Director of Home Health & Hospice Regulatory Affairs for the National Association for Home Care & Hospice says the face validity of process items is the most important information the HQRP TEP provided to CMS. “Having HOPE items and subsequent measures that actually measure what is intended is key to success,” she says.
Exclusions from Process Measures Success
Exclusions from calculating a hospice’s process measures’ success need careful consideration. Here is the list of options of which patients to exclude:
- Patient desired tolerance level for symptoms
- Patient preferences for symptom management
- Neuropathic pain
- Actively Dying (death is imminent)
- Other conditions
The report says that reassessing a symptom within two days of identifying that symptom as moderate or severe is fundamental. This is true regardless of the beneficiary’s stated tolerance-level for symptoms. It also said that process measure calculations should include patients with no symptom-management preference. Further, exclusion criteria should be the same for pain and non-pain symptoms.
Neuropathic Pain
The TEP’s recommends including neuropathic pain in the HOPE tool’s pain-reassessment process measure. Including rather than excluding patients suffering neuropathic pain prompts nurses to reassess these patients for changes. The report references research that suggests 40% of hospice patients may experience neuropathic pain. Patients who experience neuropathic pain have more severe and more distressing pain symptoms. [Tofthagen, C., Visovsky, C., Dominic, S., & McMillan, S. (2019). Neuropathic symptoms, physical and emotional well-being, and quality of life at the end of life. Supportive Care in Cancer, 27(9), 3357-3364. doi:10.1007/s00520-018-4627-x]
The TEP agrees that patients with neuropathic pain should be part of the process measure. However, they recommend excluding the same patients from the outcome measure addressing the patient’s pain impact. The report cited TEP discussion that such pain is chronic and not likely to be resolved or decreased within two days when the reassessment captures outcome data.
The TEP broadly agreed that a nurse who assesses a patient who is actively dying (life expectancy of 3 days or fewer based on clinicians’ assessment) as suffering moderate or severe pain should attempt to reassess the patient. Such patientsshould not be excluded.
The panelists agreed that process measures should include patients of all ages. Several TEP members noted that all patients experience pain and non-pain symptoms, and therefore the measures should apply to adults and children alike.
Exclusion Due to Inability to Reassess
When a hospice is unable to reassess a patient for a valid reason process measures should exclude those patients.
Identified exclusion reason were:
- discharge, alive or dead
- visit refusal
- inability to access the patient due to an emergency department or hospitalization event
- the patient traveling outside of the hospice’s service area
- inability of the hospice to contact the patient or caregiver.
However, the report says, “…hospices should be penalized if reassessment is missing or delayed due to hospice staffing or scheduling issues.”
This article is the second in a series about implementation of HOPE. Next week, Beth Noyce shares details from the panel as it discussed potential future process and outcome measure concepts.
# # #
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | Apr 11, 2024 | Admin, CMS, Regulatory
by Kristin Rowan, Editor
For a few weeks now, we have been covering the Change Healthcare cyberattack by ALPHV/BlackCat and the subsequent updates from CMS. Pharmacy and medical orders have been delayed, providers and patients are suffering, and CMS has issued “guidance” with no real solution. Underground reports indicate that Change Healthcare paid $22 million to BlackCat following the first cyberattack and that BlackCat stole 6TB of data from the system. Change Healthcare has refused to respond to questions about the alleged payment. Three weeks after the attack, Change Healthcare started to come back online, starting with the pharmacy services, which returned on March 7th. Parent company UnitedHealth Group indicated that other services would return in the coming weeks.
Legal Action
More than 87% of physicians are see more than a 20% drop in daily claim submissions. As of April 9th, physicians are still reporting issues with cash flow and anticipate higher than expected losses due to financing and loans that may be needed to cover them as the effects of the attack continue. Rivals of Change Healthcare are reportedly onboarding hundreds of customers who have left the organization. One of these, Availity, has processed more than $5 billion in claims that were left unprocessed by Change Healthcare’s system and has onboarded 300,000 providers with a backlog of more than 50 health systems waiting to start using the platform.
The attack has caused long-term disruptions, delays, cash flow problems, patient care disruptions, prescription delays, and billing issues. Some physician practices have started using personal money to cover payroll and other expenses. The US Department of Health and Human Services (HHS) has launched a formal inquiry into Change Healthcare’s data protection standards. This inquiry follows six class action lawsuits filed against the organizations. Physicians were still reporting significant impacts on their claims.
Adding Insult to Injury
Change Healthcare has barely gotten their systems up and running were still putting out fires when they were hit again.  On April 8, RansomHub contacted Change Healthcare and alleged to have 4TB of data stolen from the system and are demanding an extortion payment to keep the data private . RansomHub has threatened to sell the data, which includes US military personnel and patient data, medical records, and financial data, to the highest bidder in 12 days if the ransom isn’t paid.
On April 8, RansomHub contacted Change Healthcare and alleged to have 4TB of data stolen from the system and are demanding an extortion payment to keep the data private . RansomHub has threatened to sell the data, which includes US military personnel and patient data, medical records, and financial data, to the highest bidder in 12 days if the ransom isn’t paid.
Among the prevailing theories as to why Change Healthcare has been hit again is that the first ransom was supposed to have been split between ALPHV/BlackCat and an associate known as “notchy”, but ALPHV absconded with the ransom, leaving the other with nothing. Looking for a payout equal to what they lost, notchy partnered with RansomHub to try to recoup their losses. A second theory is that ALPHV and RansomHub are one in the same and that ALPHV went to ground after the ransom payout and have resurfaced as RansomHub. RansomHub, however, claims that after ALPHV went to ground, some of their affiliates joined the RansomHub operation and this is how they came by the data. Either way, it seems that the data stolen in the first attack was not returned after the ransom was paid and Change Healthcare is still susceptible to further extortion. This also means that the Change Healthcare system was not hacked a second time, but rather this is just an extension of the first data breach.
No word yet on whether Change Healthcare and UnitedHealth Group will pay the second ransom demand.
We will continue to follow this story and provide updates as it impacts payment and claims processing.
# # #

Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or
www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. www.therowanreport.com One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | Apr 11, 2024 | Clinical, CMS, Regulatory
By Beth Noyce, RN, BSJMC, HCS-C, BCHH-C, COQS
Home health & hospice consultant
The Hospice Outcome Patient Evaluation is a step closer to implementation.
After four years of considering options, the Technical Expert Panel (TEP) has finished its work that will inform future Hospice Quality Reporting Program results. The TEP considered quality measures to include in hospice’s future assessment tool and best choices for risk adjustment and exclusion.
The panel convened in 2019 “[we are] committed to improving the quality of care given to hospice patients,” says the 2022-2023 TEP Summary Report: Hospice Quality Reporting Program. The panel aimed to ensure that hospice quality measures are meaningful for hospice beneficiaries, transparent to hospice providers, and useful to consumers. They considered quality measures from both HOPE and claims data.
“From day one it was very clear Medicare wanted to make this a very different experience for hospice teams and make it a more valuable thing for consumers,” says Dr. Jeff McNally, Hospice Medical Director at Utah’s Intermountain Hospice,” describing his participation on the HQRP TEP. “I was actually encouraged and inspired by it,” he says. “It was the first time I had first-hand experience working with any kind of CMS entity.
“The reality is some clinicians in the field and leaders don’t have the best things to say about CMS,” he explains, but “whatever we were considering we always circled back to whether it would be burdensome to the clinical team and would it be valuable to consumers.”
The panel initially planned to meet multiple times in person, with two meetings per year and potential virtual meetings as needed. “Then COVID hit,” Dr. McNally says. “It slowed the process considerably. We never did meet again in person.”
The HQRP TEP met eight times over four years, virtually after the initial meeting. McNally described participants as coming to each meeting prepared with data and proposals for HOPE measures for which they would request input from panelists.”
From TEP recommendations early in their work, Abt Associates developed two outcome measures and two process measures in harmony with hospice’s central tenet to manage symptoms:
- Process measures:
- Timely Reassessment of Pain Impact
- Timely Reassessment of Non-Pain Symptom Impact
- Outcome measures:
- Timely Reduction of Pain Symptom Impact
- Timely Reduction of Non-Pain Symptom Impact
“The most important [recommendations] were some of the outcome measures about symptom management,” McNally explains. “What should we be helping agencies show that they’re doing well? And how do we do that? Deciding which ones, and how many symptom management measures to use and the most valuable way to show it in a fair way.”
During the past two years, TEP members prioritized which of the risk-adjustment factors suggested by Abt. Associates should apply to outcome measures and which exclusions should apply to both outcome and process measures.
The report describes risk adjustment as using statistics to exclude “confounding factors,” or elements that are outside of a hospice’s control, from calculations that could make a hospice’s performance appear either better or worse than it is. In essence, risk adjustment increases the fairness in outcome-measure calculations while exclusions do the same for both outcome and process measures.
For the outcome measures being considered, the report says that the “TEP broadly agreed that risk adjustment is very important because it accounts for external factors outside hospices’ control and more accurately reflects the quality of care provided.”
Judi Lund Person, Principal of LundPerson & Associates, LLC, agrees. “The discussion of risk-adjustment factors is vitally important to the success of upcoming process measure implementation,” says Lund Person.
Determining which risk-adjustment factors to bring to the table was not easy. “There were some nuance things that we hashed out to try and decide how to weigh some factors in risk adjustment” for outcome measures, McNally explains.
Exhibit 5 (below) summarizes the TEP’s rankings of risk adjustors suggested.
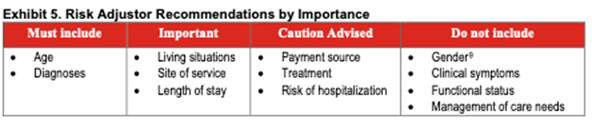
While the TEP’s priorities seem clear, the discussion concerning each risk adjustor was more complex. The TEP broadly agreed that the most important risk-adjustment factors are age and diagnosis. Some diseases are more difficult to manage than others, and patient condition tends to decline with age regardless of provider activity. Therefore, the TEP recommended that CMS adjust for these factors to ensure that common external factors do not adversely affect reported hospice care quality.
Here’s part of the nuance – the TEP also raised concerns that how well other patients with certain diseases or of certain age groups are treated might be valuable to some patients and their families seeking care for someone of the same age group or condition. Panelists fretted over possibly obscuring that information for consumers seeking hospice care by adjusting for those risk factors.
Living situation as a risk adjustor ranked as important to TEP members because hospices have no control over what level of assistance is available to patients. Similarly, site of service ranked high as a risk adjustor because, said some panelists, care is delivered very differently across settings, and patients and/or caregivers tend to provide higher hospice satisfaction ratings for hospices in home settings than for those in facilities,” according to the report.
Lund Person, who is also former Vice President of Regulatory and Compliance at the National Hospice and Palliative Care Organization (NHPCO), notes that the TEP recognized living situation and site of service as “important” risk adjustment recommendations.
“Identifying site of service will help to distinguish between care at home and care in a facility,” she says. Also vital, she continues, “is the recommendation from the TEP to consider length-of-stay as a risk-adjustment factor, including the differences between a 4-day length of stay and a 6-month length of stay.”
One TEP member cautioned that using payment sources, IV therapy, and risk of hospitalization as risk adjustors might tempt some hospices to use them to distort a hospices’ apparent care quality.
TEP members did not recommend using as risk adjustors gender, clinical symptoms, functional status and management of care needs. They did not discuss why they rejected gender, but several agreed that using clinical symptoms would not be of value because of their high correlation with diagnoses. Because hospice providers typically see hospice patients decline in ADL and IADL abilities, and hospice goals are focused on comfort rather than functional improvement, functional status was on the TEP’s “Do Not Include” as a risk adjustor list. And finally, one TEP member strongly opposed adjusting for patients’ medication management, supervision or safety assistance needs (management of care needs), explaining that “the public and CMS should hold hospices accountable for planning around oral medication, injectable medication management, and supervision and safety assistance,” the report says.
The TEP did suggest that using some risk adjustment factors as part of the HQRP could assist hospices internally with quality improvement while others would be more valuable to patients and families. For example, Patients and families would benefit from more straightforward risk adjustment that helps them select a hospice,” the report says, “including factors such as diagnosis. For publicly reported data used to select a hospice, the TEP suggested using demographic factors (including age but excluding gender), socioeconomic factors, living situation, and diagnoses.”
Dr. McNally hopes eventually to use HPRP data to promote Intermountain Hospice’s care. Intermountain Hospice is part of Intermountain Health, a health care provider with presence in multiple states. “You can’t take the current metrics to doctors’ offices and families to show anything meaningful,” he says. “It’d be great to have metrics we could take to our neurology docs and other docs,” he says. “I really think we provide better care and more options when patients stay within our system.
This article is the first in a series about implementation of HOPE. Next week, Beth Noyce shares details from the panel as it evaluated process measures.
# # #
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | Apr 4, 2024 | CMS, Regulatory
By Kristin Rowan, Editor
On March 28, CMS issued a new proposed rule to update Medicare hospice payments. Here’s what we know.
The new proposed rule:
- Would change the existing hospice wage index
- Clarifies current policy related to the hospice “eletion statement” and the “ntoice of election”
- Adds clarifying language around hospice certification
- Includes a request for information to get comments on implementing a separate payment mechanism for high-intensity palliative care services
- Proposes that Hospice Quality Reporting Program (HQRP) measures be collected through the Hospice Outcomes and Patient Evaluation (HOPE), adding two new measures
- Also proposes changes to the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Hospice Survey
The new proposed rule includes a net 2.6% increase in payments over FY 2024. This includes a 3% market-based update, and a 0.4% cut for productivity. Submitting quality data is a requirement of the net pay. Hospices that do not submit quality data will be penalized 4%, netting a 1.4% decrease in payments. The propsed rule for 2025 is .5% lower than the 2024 hospice payment increase.
The National Hospice and Palliative Care Organization (NHPCO) says the rate increase is good, but not high enough. NHPCO COO and Interim CEO, Ben Marcantonio said, “To continue providing the high level of care our patients and their families deserve, hospices require a payment rate that accurately reflects the current economic challenges. We know that hospice care has demonstrated $3.5 billion in annual savings for Medicare, which underscores the critical importance of investing in hospice to ensure continued beneficiary access to quality end-of-life care.”
Palliative Care
CMS is interested in feedback and proposals from hospice agencies for providing complex palliative treatments and high-intensity hospice care when that care negatively impacts hospices financially. CMS aims to care for high-cost patients through palliative care rather than acute care. The NHPCO agrees with the CMS proposal to fund palliative care separately from standard hospice or acute care. CMS will take feedback and proposals through May 28, 2024. Comments can be submitted electronically at http://www.regulations.gov, by following the “Submit a Comment” instructions. Comments can also be sent by regular or express mail. Addresses can be found in the full proposed rule. Follow the search instructions at http://www.regulations.gov to see all submitted comments.
The proposed rule can be viewed starting April 4, 2024 at the Federal Register at https://www.federalregister.gov/public-inspection.
# # #
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com









