by Kristin Rowan | May 10, 2024 | Admin, Caring for the Caregiver, Clinical, Marketing, Recruitment & Retention, Regulatory
by Kristin Rowan, Editor
I was honored to have been a guest on Health Futures – Taking Stock in You Radio Show on Money Radio 1510 AM discussing navigating the home care revolution. Health Futures is hosted by HomeCare expert Bob Roth, owner of Cypress HomeCare Solutions. Cypress just celebrate its 30th anniversary last week and is the recipient of a Grant to Innovate within Medicaid in partnership with PocketRN and is the 2013 & 2018 winner of the BBB Torch Awards for Ethics. You can listen to the full radio show here. Below is the blog based on the show, written by the CEO of Strait Talk PR, Lauren Strait.
by Lauren Strait, CEO Strait Talk PR
The Aging Population Tsunami
By 2050, the 85-year-old population in the United States is expected to quadruple. As this massive demographic shift unfolds, the already strained home care industry will face unprecedented challenges in meeting the escalating demand for quality care services.
Bob Roth, Managing Partner of Cypress HomeCare Solutions, recently had Kristin Rowan, of The Rowan Report on the radio show and podcast to discuss this trend and everything a consumer needs to know about the homecare industry and how it will affect them.
A Trusted Voice Amid Industry Upheaval
In the latest episode of “Health Futures, Taking Stock in You” hosted by Bob Roth of Cypress Homecare Solutions, Kristin Rowan, Owner and Editor of The Rowan Report, offered insights into how her publication is guiding the industry through this seismic transition.
The Rowan Report’s Unbiased Expertise
What began as a print magazine reviewing home health technology has evolved into a comprehensive digital hub covering regulatory updates, workforce solutions, marketing strategies, and groundbreaking innovations. Rowan emphasized the publication’s commitment to neutrality when evaluating new products and services.
“We do our best to remain as neutral as possible…that’s one of the things that Tim [her father and the founder] established early on in his relationships with tech providers.”
Empowering a Strained Workforce
With a redesigned website offering robust search capabilities, The Rowan Report curates resources to help agencies streamline operations and alleviate administrative burdens on overstretched staff. “The solution is not more people because they’re just not there,” Rowan stated. “But the solution is collaboration to better utilize the people that you have.”
The publication explores leveraging AI, voice technologies, automated claims processing, and outsourcing to reduce paperwork and maximize efficiency, enabling care professionals to concentrate on frontline patient care.
Preparing for the Age Wave
As the population ages, The Rowan Report recognizes the need to educate professionals and families on navigating the complexities of long-term care. By convening experts, the publication covers crucial topics like choosing providers, understanding Medicare/Medicaid, and planning for future care needs.
An Indispensable Industry Guide
With over 25 years of experience, The Rowan Report stands as an indispensable guide for the home care industry as it braces for the challenges and opportunities of an aging America. Access their insights at www.therowanreport.com.
Bob Roth is Managing Partner of Cypress HomeCare Solutions. He assisted in creating Cypress HomeCare Solutions with his family in 1994. Bob brings the depth and breadth of his nearly 36 years of consumer products, health care and technology experience to the home care trade. Over the years, Bob has received a number of awards. These include the January 2014 CEO of the Month and finalist for the 2015 Phoenix Business Journal’s Healthcare Heroes award. Cypress won the Better Business Bureau’s Business Ethics award in 2013 and 2018.
In March 2017, Arizona Governor Bob Ducey appointed Bob to the Governor’s Advisory Council on Aging. This was the first time in the Council’s 40 years that a home care/home health care agency owner/manager has served on the Council. Nationally, Bob serves on the Board of Directors for the Home Care Association of America (HCAOA). Locally, he serves on the Board of Directors for DUET Partners in Aging. Additionally, he is on the ambassador committee for Aging 2.0 – Phoenix Chapter. On September 11, 2019 Bob won the Home Health Care News Future Leader Award. The award recognizes up-and-coming leaders elevating the home health industry. When he’s not working, Bob enjoys spending time with his wife Susie, their three daughters, and playing golf, tennis, hiking and walking with Ruby and Lacey, our pet therapy dogs.
Bob Roth is Managing Partner of Cypress HomeCare Solutions. He assisted in creating Cypress HomeCare Solutions with his family in 1994. Bob brings the depth and breadth of his nearly 36 years of consumer products, health care and technology experience to the home care trade. Over the years, Bob has received a number of awards. These include the January 2014 CEO of the Month and finalist for the 2015 Phoenix Business Journal’s Healthcare Heroes award. Cypress won the Better Business Bureau’s Business Ethics award in 2013 and 2018.
In March 2017, Arizona Governor Bob Ducey appointed Bob to the Governor’s Advisory Council on Aging. This was the first time in the Council’s 40 years that a home care/home health care agency owner/manager has served on the Council. Nationally, Bob serves on the Board of Directors for the Home Care Association of America (HCAOA). Locally, he serves on the Board of Directors for DUET Partners in Aging. Additionally, he is on the ambassador committee for Aging 2.0 – Phoenix Chapter. On September 11, 2019 Bob won the Home Health Care News Future Leader Award. The award recognizes up-and-coming leaders elevating the home health industry. When he’s not working, Bob enjoys spending time with his wife Susie, their three daughters, and playing golf, tennis, hiking and walking with Ruby and Lacey, our pet therapy dogs.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or
www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | May 10, 2024 | Admin, Caring for the Caregiver, Clinical, Regulatory
by Kristin Rowan, Editor
Last week, we reported on the proposed Bill in the Connecticut Senate and House to provide additional precautions for home care worker safety. In wake of the  Joyce Grayson murder during a home health visit, leadership in Connecticut aimed to safeguard home health and home health aide workers and collect risk assessment data on the same.
Joyce Grayson murder during a home health visit, leadership in Connecticut aimed to safeguard home health and home health aide workers and collect risk assessment data on the same.
On May 6, 2024, CT legislature passed bills in both the Senate and House of Representatives. Instead of the proposed bills that we reported on previously, both branches added amendments to previous bills. The bills include provisions for cyberattack readiness, child safety, and other items not related to care in the home.
First Stage of Home Care Worker Safety
Some of the provisions in the final bill are effective July 1, 2024. As we previously reported, hospice agencies are currently exempt from these provisions and the CT legislature will address hospice agencies in their next session.
On and after July 1, 2024
The Commissioner shall increase the fee payable to a home health care or home health aide agency that provides escorts for safety purposes to staff conducting a home visit to cover the costs of providing such escorts.
The Commission of Public Health will establish and administer a home care staff safety grant program to provide grants to home health and home health aide agencies for staff safety technology, including, but not limited to :
- A mobile application for staff to access safety information about a client
- A method for staff to communicate with either local police or other staff in the event of an emergency
- A global positioning system-enabled, wearable device that allows staff to contact local police
Effective July 1, 2024
The sum of one million dollars is appropriated to the Department of Public Health for the the fiscal year ending June 30, 2025, to establish and administer the aforementioned grant program.
The Commissioner of Public Health and the Commission on Community Gun Violence Intervention and Prevention, will develop or find educational material about gun safety practices and provide such to primary care providers to give to patients who are 18 years of age or older.
Second Stage of Home Care Worker Safety
Some of the provisions in the final bill are effective October 1, 2024. Home health and home health aide agencies have five months to comply with these measures.
Effective October 1, 2024, home health and home health aide agency must collect and provide to assigned workers information about:
The client, including as applicable;
- psychiatric history
- history of violence
- history of substance use
- history of domestic abuse
- current infections, if any, and treatment received
- whether diagnoses or symptoms have remained stable over time
Other persons present or anticipated to be present at the location of care including, if known to the agency:
- name and relationship to client
- psychiatric history
- history of violence or domestic abuse
- criminal record
- history of substance use
Location where employee will provide services including, if know to the agency:
- the crime rate for the municipality in which employee will provide services
- the presence of any hazardous materials, including, but not limited to used syringes
- the presence of firearms or other weapons
- the status and of the fire alarm system
- the presence of any safety hazards, including, but not limited to, electrical hazards
By October 1, 2024, each home health and home health aide agency must:
Provide staff training consistent with the health and safety training curriculum for home care workers, including but not limited to:
- Training to recognize hazards commonly encountered in home care workplaces
- Applying practical solutions to manage risks and improve safety
Conduct monthly safety assessments with each staff member and
Provide staff with a mechanism to perform safety checks, which may include, but need not be limited to:
- A mobile application that allows staff to access safety information about the client
- A means of communicating with local police or other staff in the event of an emergency
- A global positioning system-enabled, wearable device that allows staff to contact local police by pressing a button or through another mechanism
Effective October 1, 2024
Each home health and home health aide agency shall, in a manner prescribed by the Commissioner of Public Health:
- Report each instance of verbal abuse that is perceived as a threat or danger to the staff
- Report each instance of physical, sexual, or any other abuse by a client against a staff member
Third Stage of Home Care Worker Safety
No later than January 1, 2025
Beginning January 1, 2025 and annually therafter, the commissioner shall report to the joint standing committee:
- The number of reports of violence and abuse received
- The actions taken to ensure the safety of the staff member about whom the report was made
Effective January 1, 2025
Each individual health insurance policy shall provide coverage for escorts for the safety of home health care agency or home health aide agency staff
The joint standing committee of the General Assembly will convene a working group to study staff safety issues affecting home health and home health aide agencies, including but not limited to the following members:
- Three employees of a home health care or home health aide agency
- Two representatives of a home health care or home health aide agency
- One representative of a collective bargaining unit representing home health care or home health aide agency employees
- One representative of a mobile crisis response services provider
- One representative of an assertive community treatment team
- One representative of a police department; and
- One representative of an association of hospitals in the state
As we mentioned before, these regulations will become mandates across the country soon. OSHA has found the home care agency in Connecticut at fault for failing to implement safety procedures and precautions in the death of Joyce Grayson. The nurse’s family is suing the home health agency for wrongful death. Connecticut has established a protocol for safety measures, committees, reporting, and grant programs to implement immediate safety procedures across home health and home health aide agencies in the state. Before these provisions are passed on a national level, and before you have to tell the family of one of your staff that they aren’t coming home…
We urge you to:
- Create a safety committee within your agency
- Invest in training on de-escalation, workplace violence prevention, and self-defense
- Research and invest in a GPS-enabled emergency alert system for your staff. We recommend POM Safe and Katana Safety
- Insist on background information on all clients and others living in the home upon intake and BEFORE the first home visit
- Create a safe and comfortable way for your staff to report verbal abuse, violence, or uneasiness from any in-home visit
- Invest in escort and/or paired visits for high-risk clients, first-time clients, or any other situation that warrants it
We will continue to follow this story and provide updates as we receive them.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | May 10, 2024 | M&A
Bon Secours Mercy Health to Outsource Home Health and Hospice to Compassus
Bon Secours Mercy Health (BSMH), the fifth-largest Catholic health system in the U.S., and Compassus, a leading national provider of home-based health care services, announced on May 2 that they have signed an agreement to form a 50/50 joint venture partnership for BSMH home care and hospice. Under the agreement, Bon Secours will outsource to Compassus, who will manage operations for 10 home health agencies and 11 hospice operations spanning five states.
Under the agreement, BSMH will maintain ownership of its existing hospice house real estate assets in specific locations while Compassus will manage the operations. BSMH will work closely with Compassus to support the home health and hospice associates transferring to employment with Compassus. Under the joint venture, the team will continue to provide spiritually grounded care and will operate in accordance with Ethical and Religious Directives.
The agreement is subject to state and federal regulatory review and final diligence; however, the agreement formalizes the intent of both parties to move forward with the transition and integration.
About Compassus
 Compassus provides home-based services including home health, infusion therapy, palliative and hospice care. The company’s more than 6,000 team members serve more than 100,000 patients annually across more than 250 locations in 29 states. This is not the company’s first joint venture. In 2020, Compassus became managing partner of Ascension at Home, a joint venture between Ascension and Compassus.
Compassus provides home-based services including home health, infusion therapy, palliative and hospice care. The company’s more than 6,000 team members serve more than 100,000 patients annually across more than 250 locations in 29 states. This is not the company’s first joint venture. In 2020, Compassus became managing partner of Ascension at Home, a joint venture between Ascension and Compassus.
About Bon Secours Mercy Health
Bon Secours Mercy Health (BSMH) is one of the 20 largest health systems in the United States and the fifth-largest Catholic health system in the country. The ministry’s quality , compassionate care is provided by more than 60,000 associates serving communities in Florida, Kentucky, Maryland, New York, Ohio, South Carolina and Virginia, as well as throughout Ireland.
, compassionate care is provided by more than 60,000 associates serving communities in Florida, Kentucky, Maryland, New York, Ohio, South Carolina and Virginia, as well as throughout Ireland.
Bon Secours Mercy Health provides care for patients more than 11 million times annually through its network of more than 1,200 care sites, which includes 48 hospitals. In 2022, BSMH provided more than $600 million dollars in community investments across five states, ensuring that cost is not a barrier to health care for patients in need.
In addition to charity care, BSMH invests in programs that address chronic illness, affordable housing, access to healthy food, education and wellness programs, transportation, workforce development and other social determinants of health. The Mission of Bon Secours Mercy Health is to extend the compassionate ministry of Jesus by improving the health and well-being of its communities and bring good help to those in need, especially people who are poor, dying and underserved. https://bsmhealth.org/
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Elizabeth E. Hogue, Esq. | May 2, 2024 | Clinical
by Elizabeth E. Hogue, Esq.
Noora Health has developed a program of “health companions” in a variety of types of healthcare settings (“Teaching Patients How to Heal,” The New York Times, April 14, 2024) to help patient heal. The basis of these programs is that when medical information is properly communicated to patients and their families, complications of surgeries and illnesses are reduced. An added bonus is that acts of violence by frustrated family members against health care workers are reduced.
If patients are most comforted by their loved ones, why not involve them in the healthcare process? “We realized that caregivers get little to no guidance within the health care system,” said Shahed Alam, a co-founder of Noora Health. Many patients do not know why they are receiving care. Doctors and nurses tend repeat the same information to patient after patient.
“We realized that caregivers get little to no guidance within the health care system,” said Shahed Alam, a co-founder of Noora Health. Many patients do not know why they are receiving care. Doctors and nurses tend repeat the same information to patient after patient.
In institutional settings, staff nurses literally take over the floors to teach patients and their family members. On cardiac floors, for example, staff nurses tell patients how to cough without stressing their hearts, how to scratch without adversely affecting their wounds, and how pacemakers work. Staff nurses also help patients sift through good and bad information. Classes frequently include how to manage side effects of medications and the importance of handwashing.
Many patients and their family members come to view the staff nurses as therapists, coaches, friends and philosophers all rolled into one. A family member who received help from a health companion described the companion as a “friend” without whom she would not have been able to care for her family member.
Although home care providers, including Medicare certified home health agencies, hospices, private duty home care agencies, and durable medical equipment (DME) companies do not necessarily have a “captive audience” like institutional providers, it is still possible to utilize health companions. Field staff can be trained to provide teaching that is similar to that provided by health companions. Teaching from health companions may also be provided to home care patients and their family members in group settings. Hospices may, for example, provide volunteers to be with patients while their caregivers attend. And, of course, virtual teachings with health companions may also prove valuable.
Providers often consider ways to differentiate their services in a competitive marketplace. Perhaps the use of health companions is one way to do so, Providers may also enhance loyalty from patients and their families, improve quality of care and prevent emergency room visits, hospitalizations and rehospitalizations. Think about it!
©2024 Elizabeth E. Hogue, Esq. All rights reserved.
No portion of this material may be reproduced in any form without the advance written permission of the author.
©2024 This article appeared in The Rowan Report. All rights reserved.
by Kristin Rowan | May 2, 2024 | Product Review
by Kristin Rowan, Editor
Revenue Cycle Management (RCM) addresses several pain points for care at home agencies: coding errors, timely reimbursement payments, and employee workload. Available as both full-service and SaaS products, RCM automation offers higher reimbursement rates, lower overhead costs, and overall better efficiency for your agency. Not having a RCM tool leaves your agency at higher risk for nonpayment, audits, and lengthy revenue cycles that impede your ability to manage your agency’s revenue.
Last week, I had the opportunity to talk with Michael Greenlee, Founder and CEO of HealthRev Partners. Hannah Vale, Chief Strategy Officer, joined him on the call. They told me about the HealthRev Partners’ launch of their new RCM tool, Velocity.
About HealthRev Partners
HealthRev Partners offers OASIS & POC Review and Coding assistance to home health, hospice, and palliative care agencies. The partnership program starts with an initial telephone conference, followed by a live review of documentation with an OASIS expert with recommendations for accuracy and compliance. Additionally, they have a precepting partnership program to enhance clinician performance and documentation practices. The RN guided program offers OASIS documentation review and correction sessions to ensure accurate and compliant documentation. Their solutions aim to maximize reimbursements with faster turnaround and higher accuracy.
HealthRev Partners Launches Velocity
On April 1, 2024, HealthRev Partners announced the launch of a new SaaS solution for Revenue Cycle Management, Velocity. HealthRev Partners designed Velocity to transform RCM for multi-site agencies. In addition to RCM, the tool offers operational insights for optimization and growth. Velocity focuses on real-time analytics and operational efficiency by centralizing data between locations. If you have an in-house RCM team, Velocity can be a stand-alone SaaS. However, if you need it, it can also be a full-service solution with outsourced coding and RCM experts on the Velocity team.
About Velocity
According to Michael Greenlee, many agencies lack tracking of their aging accounts receivable and the status of their claims. Without these, agencies can be leaving hundreds of thousands of dollars stuck in the revenue cycle without ever getting reimbursement from the claim. Velocity works with any existing EMR to pull data from coding and billing information. The built-in quality assurance (QA) solution is automated and customizable for charting and documentation. HealthRev Partners launched Velocity to help agencies overcome some of the pain points agencies have with RCM, billing, and coding.
Features
- Productivity and Accountability Reporting: Whether using Velocity as an outsourced solution or SaaS, instantly see time-stamped productivity reports, accuracy reports, and clinician QA scoring
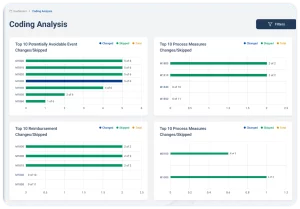
- Ai powered tracking: All claims in the 61-90 day and over 90 day segments are brought into the system for tracking with a follow-up reminder for each claim, payment information, and reasons for nonpayment.
- Claims forecasting: Velocity shows the current financial status of the agency, and with enough data in the system, can provide revenue forecasts simply by entering a future date into the reporting system.
- Pre-built database: All charting codes are built into the system and are searchable by keyword or phrase to reduce coding errors and increase reimbursement rates
- Platform agnostic: For many agencies, switching to a different EMR system costs more than the sticker price on the solution. With Velocity, there is no loss of data because it holds previous EMR data when you switch.
- Advanced Funding: Partners with Velocity have access to their AR funds before claims are processed, with an immediate credit line of up to $100,000, or 80% of the agencies AR.
Differentiation
Whether you need a software solution for your in-house RCM team or are looking to outsource your billing and coding to a partner, choosing the right RCM team is essential for your success. With so many RCM companies available in the market, it can be difficult to choose the right one. To choose the right RCM partner, there are a few factors to consider:
How does the solution or company match with the mission and vision I have for my agency?
HealthRev Partners has an “aspiration to develop innovative solutions that create boundless opportunities for our clients to advance their mission.”
Does the solution have the right tools for my success?
The analytics tools in Velocity can by customized to each agency’s KPIs. Velocity offers a fully supported software solution, a SaaS solution, and everything in-between to provide each agency with the level of support they need to succeed. Clinician productivity reports calculate clinician reimbursement by month. This shows which of your clinicians needs additional training and which should be recognized for their achievements, which can help to decrease your turnover rates. Velocity will custom build additional dashboards and measurements, included in the cost of the software.
Is the software solution safe for my agency and my clients?
Velocity is a HIPAA secure platform and is undergoing SOC-2 certification to protect your organization and the privacy of your patients.
Does the software partner have my best interests in mind?
Have you ever talked to someone who is so passionate about what they do that their energy is contagious? That was my experience in talking with Michael Greenlee, CEO and Founder of HealthRev Partners. Our one-hour scheduled software review meeting turned into a two hour conversation about what Velocity is designed to achieve. We also talked about how much potential it has to help home health, hospice, and palliative care agencies to survive.
Greenlee’s goal for Velocity is to have 0 claims go past 90 days for any agency they work with. They train each of their team members to meet the needs of an individual customer before they touch the account. HealthRev Partners offers “white glove service” to make good agencies great and to help partners dominate their marketplace. Michael partners with agencies he believes in as much as he believes in his own company. “We’re passionate about securing success for home health, hospice, and palliative care agencies across the nation.”
Future Considerations
Michael, Hannah, and I talked at length about what might be possible with Velocity. (So much so that Hannah asked if I was available to attend their next planning meeting.) AI capabilities are evolving and maturing at a rapid rate. Generative AI will become the standard for software solutions in care at home in short order. Michael’s passion for elevating the efficiency and prosperity of his home health, hospice, and palliative care agency partners will undoubtedly lead to even more innovation. Hannah Vale offered, “Our goal is to further enhance the sophistication of the AI. We consistently heed client feedback to creatively address their evolving requirements.”
To book a demo with HealthRev Partners, click here.
# # #
 Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. Additionally, she has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. Additionally, she has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Kristin Rowan | May 2, 2024 | Clinical, Regulatory
Home health agency failed to protect Joyce Grayson
History
We’ve been following the story of Joyce Grayson since her death in October of 2023. The news was first published in The Rowan Report here on November 8th, 2023.On April 14th, we reported on the pending Senate Bill in Connecticut that would require home health agencies to provide additional information and safety precautions prior to a home visit. The safety of solo workers is now even more important to home health and hospice agencies with the most recent update.
Today
May 1, 2024, the U.S. Department of Labor (DOL) posted a news release on their investigation into the death of Joyce Grayson, a home health nurse in Connecticut. According to the Department of Labor, OSHA has determined that Elara Caring exposed their employees to workplace violence from patients who were known to pose a risk to others. Jordan Health Care Inc. and New England Home Care Inc., both doing business as Elara Caring, have been cited for willful violation of the agency’s general duty clause. OSHA cited them for not developing and implementing safety measures to protect employees from workplace violence. They also cited the agency for failure to report work-related injury and illness records within four business hours.
Repercussions
OSHA has proposed more than $163,000 in penalties against Elara Caring. Elara Caring has 15 days from receipt of the citations to respond, request a hearing, or contest the findings.
“Elara Caring failed its legal duty to protect employees from workplace injury by not having effective measures in place to protect employees against a known hazard and it cost a worker her life,” said OSHA Area Director Charles D. McGrevy in Hartford, Connecticut. “For its employees’ well-being, Elara must develop, implement and maintain required safeguards such as a comprehensive workplace violence prevention program. Workplace safety is not a privilege; it is every worker’s right.”
OSHA found that Elara Caring could have reduced the potential for workplace violence by looking at the root causes of violent incidents and “near misses.” They could also have provided clinicians with background information on patients prior to a home visit. Other recommendations from OSHA include providing emergency panic alert buttons and using safety escorts for visits with high-risk patients.
Future Recommendations
The DOL states that employers should have a comprehensive workplace violence program. This program should include both management and employee involvement. Further, the DOL says this plan should have a written program with a committee. Elements of a workplace violence program include:
- Analysis of a home upon new patient admission
- Hazard prevention and control
- Training and Education
- Resources for Impacted Employees
- Recordkeeping
- Employee Feedback
Implications
If Elara Caring is fined for failure to keep their clinicians safe as a result of the investigation into Joyce Grayson’s murder, state and national level regulations are sure to follow. However, even if the laws in your area don’t change, investing now in workplace safety for your clinicians could save you from similar allegations and fines. As we mentioned in last week’s article about the Senate Bill, we have been in touch with several emergency alert companies and will be providing product reviews in the next few weeks. Start a workforce safety committee, develop a written plan for mitigating dangerous situations, and issue emergency response systems to all of your clinicians before it is your agency under investigation. More importantly, take these steps before your team loses one of its own to workplace violence.
# # #
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | Apr 26, 2024 | Admin, Clinical, CMS, Regulatory
by Johnathan Eaves, Senior Director of Communications, Axxess
Treating Medicare patients comes with a level of nuance that is important to understand to ensure that organizations remain compliant and patients receive appropriate care. Standards for quality care and payment can sometimes be dictated by Medicare’s payment policies and at other times be decided by the Conditions of Participation. There is an important difference between these two governing principles that providers should understand to ensure compliance.
Care at home industry veteran and Axxess Senior Vice President of Clinical Services Arlene Maxim RN, HCS-C, offered insights into the differences between Medicare’s policy and its Conditions of Participation during a recent webinar.
Explaining the Difference
Maxim pointed out that the differences between policy and the conditional requirements comes down to what can be billed and what are the quality standards for the services provided.
“The Conditions of Participation are dealing primarily with quality, whereas Medicare policy is related to payment,” said Maxim. And while there is a difference, that doesn’t mean both aren’t important and must always be followed.
“If Medicare policies are not followed, you are audited and if you do not have documentation to support those policies, you’re not going to get paid,” said Maxim “Oftentimes, with PDGM, staff members are not getting past that first 30 days. They’re not understanding what they need to do to keep that patient who continues to qualify for services on for longer.”
Maxim says that the problem is often that clinicians do not understand Medicare policy. “Every piece of documentation we submit to the Medicare program for review [needs to be] as pristine as we can possibly get it,” she said.
Assessment and Documentation
Proper assessment and documentation is something Maxim feels is critical in ensuring quality care, meeting Medicare requirements, and receiving payment for services.
“Complete and detailed documentation is going to be the key for agency payment by the Medicare program,” Maxim said.
Maxim pointed out certain services covered under Medicare policy may include observation and assessment, management and evaluation of a care plan, maintenance therapy, teaching and training activities, administration of medications, wound care, ostomy care, rehab nursing, venipuncture, skilled nursing visits, and more.
She also cautioned that agencies need to be prudent with the funds they receive from Medicare, viewing them as a potential “short-term, interest-free loan” until undergoing any audit. Until their documentation is reviewed and approved, there are no guarantees.
“Medicare is an insurance and it’s not free,” said Maxim. “Medicare policy provides us with a list of covered items. If experiencing an audit, and if the documentation is not there to cover the covered service, you’re not in compliance with that Medicare policy and you will not be paid for the services.”
Communicating With Physicians
Maxim further emphasized the importance of frequent contact with physicians, adherence to care plans, and ensuring that care plans are simple with individualized plans and goals that are achievable.
“You want to make sure that you have orders that physicians are actually going to read and to determine that they make sense and they’re going to sign off on them,” said Maxim.
“Keep your plan of care simple.”
# # #
Axxess Home Health, a cloud-based home health software, streamlines operations for every department while improving patient outcomes.
© 2024 Axxess. For reprint permission, please contact The Rowan Report: kristin@therowanreport.com
by Kristin Rowan | Apr 26, 2024 | CMS, Recruitment & Retention, Regulatory
by Kristin Rowan, Editor
The Centers for Medicare and Medicaid Services (CMS) has finalized the “Ensuring Access to Medicaid Services” rule, more commonly known as the 80/20 rule. The 80/20 finalized rule requires at least 80% of Medicaid payments for home care services goes to caregiver wages. No more than 20% can be spent on administrative or other overhead costs. The White House, citing a study by The Commonwealth Fund, says that higher wages for caregivers will reduce turnover. Facing massive workforce shortages, home health, hospice, and supportive care at home agencies have been struggling to recruit and retain an adequate number of caregivers. The higher wage will also increase the quality of care, according to the study.
Prior to the 80/20 rule, there was no law or rule requiring home care agencies to report how they were spending money from federal medical payments. The rule includes requirements for states to create advisory groups to consult on rates and compensation. This changes the current Medical Care Advisory Committee regulations by increasing the percent of beneficiaries on the committee from 10% to 25% over the next two year. The Home Care Association of America (HCAOA) and the National Association for Home Care & Hospice (NAHC) argued that the rule adds administrative requirements to home care agencies while simultaneously reducing the resources available to fund them. NAHC President Bill Dombi said, “We all agree that more needs to be done to support the direct care workforce; however, this policy will make things worse, not better.” NAHC suggests the policy will force some agencies to close and others will leave the Medicaid program altogether, causing patients to have even more problems accessing care.
From the text of the final rule, CMS acknowledges additional comments that the minimum direct payment to caregivers in this rule will create hardships for some agencies. Across the country, there are substantial differences among waiver programs for HCBS that are not accounted for in the rule. There is some flexibility built into the rule to account for these factors, according to CMS. Some of the flexibilities include:
- Excluding some costs from the calculation
- Including clinical supervisors in the calculation
- Allowing states to set a different minimum for small providers
- Allowing states to develop their own criteria to qualify as a small provider
- Allowing states to develop criteria to exempt some providers from the rule
- Exemption from the minimum payment rule for all Indian Health Service and Tribal health programs
The final rule also changes the timeline for complying with the rule from four years after the date of publication to six.
Other comments included the need to address various reasons for the workforce shortage. In addition to low wages, commenters cited the social valuation of direct care work, lack of governmental support for some workforce pipelines, and immigration policies as deterrents to recruitment. One suggested that CMS start looking at creative strategies for developing an atypical workforce.
There were several submitted comments stating the either HHS or CMS or both does not have the authority under the Affordable Care Act to make specific requirements for minimum payments, but only to ensure that each State is assessing payment regulations and ensuring payments are economical, efficient, and ensure quality of care. A specific section of the Affordable Care Act, section 2402(a)(1) requires the Secretary of the Department of Health and Human Services (HHS) to ensure states implement service systems to allocate resources. The provision does not give HHS the authority to dictate the terms of those service systems, only to ensure the states develop those systems. Not surprisingly, CMS disagreed with those comments.
Many people questioned the 80% as being unrealistic, too high, and not based on quality data. CMS cited data from several states, who have pass-through requirements of 80-95% for all rate increases. This is not a minimum payment from all Medicaid payments, only a requirement for a minimum pass-through to direct care workers of increases in rates. Two states, Minnesota and Illinois, currently have minimum payment requirements set at 72% and 77%, respectively. CMS used these two states as justification for the 80% rule, acknowledging that it is higher than both states while also acknowledging that they did not perform a state-by-state study of the impact the 80% rule will have. CMS states the rate was set higher than those states to “encourage further steps towards improving compensation for workers.” CMS believes that requiring HCB agencies to pay their direct care workers a higher percentage of Medicaid rates than any state currently does will somehow make those agencies want to voluntarily pay even more.
The 80/20 Rule and Technology
Technological advances in telehealth, remote patient monitoring, revenue cycle management, scheduling, employee benefits, assistive technology, EVVs, EMRs, CRMs, and other software solutions can and will lower overhead costs and increase efficiency in your agency. Paperwork automation can reduce the time spent on documentation by a significant percentage. Revenue Cycle Management software can reduce claim denials and decrease reimbursement payment cycles so you can get your money faster. They can also reduce the number of unpaid claims. Employee benefit and training software can reduce responsibilities for HR teams, lessen the requirements for clinical supervisors, and cut training time in half, getting your newly recruited caregivers out in the field faster. Scheduling and onboarding software can increase your intake capabilities. The advances in generative AI allow you to create robust reports almost instantly so you can see your agency’s strengths and weaknesses and create plans for improvement.
Some of these costs will be excluded from the calculations for the 80% rule. Now is the time to invest in technology for your agency. Not only will your agency be more efficient and more effective, but you will be able to care for more patients with the same staff you have now, and the software solutions are as close to cost-neutral as they will ever be. We have a list of technology solutions that we’ve recently discovered and will be writing about in the next few weeks. If you are in immediate need of a software solution, contact us directly for a consultation.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | Apr 26, 2024 | CMS, Medicare Advantage, Regulatory
By Beth Noyce, RN, BSJMC, BCHH-C, COQS
CHAP-certified home health & hospice consultant
This is part 3 of the 3 in the series, outlining the discussions and implications in adopting new outcome and process measures for Hospice care. The final segment addresses future process and outcome measures that the board discussed, but did not yet implement. Read Part 1 on Outcome Measures and Part 2 on Process Measures.
The TEP discussed potential future process and outcome measure concepts that Abt Associates presented to the panel as well.
The process measures included:
- Education for Medication Management
- Wound Management Addressed in Plan of Care
- Transfer of Health Information to Subsequent Provider
- Transfer of Health Information to Patient/Family Caregiver
Hope-based outcome measures were:
- Patient Preferences Followed throughout Hospice Stay
- Hospitalization of Persons with Do-Not-Hospitalize Order
Developing education for medication management as a process measure was a popular concept, and the top priority of the recommended measures with the TEP as they “broadly agreed that CMS should develop this measure,” the report says, citing “a significant need for training in medication management for patients and their caregivers.” They recommended that the measure weigh more heavily when care is provided in a home setting than in a facility setting because hospices are unable to control facility training and hiring practices. One panelist commented that including the phrase “during today’s visit” in the measure is important.
Whether CMS should further develop the process measure addressing wound management in the plan of care was less straight-forward, as panelists provided varied feedback. They generally agreed that this measure is important, as having a record of wound management addressed in the plan of care can hold the staff accountable for treating the wounds. But some members recommended measuring wound management with outcome measures rather than process measures. One panelist cited potential problems from patients’ deterioration over time and another noted that the time frame of this measure is important, and encouraged recording the process of getting care in place once a wound is identified. The panel agreed CMS should carefully define the measure’s specifications.
Because standard practice for most agencies is, when a patient is discharged live, to transfer health information to the subsequent provider and to the patient and family or caregiver, TEP members expressed that the two measures were likely to “top out,” meaning they would almost always be marked “Yes,” making them of no value in differentiating between hospice providers. The group generally discouraged developing these process measures.
The group strongly rejected any merit in developing two outcome measures concerning Patient Preferences Followed Throughout Hospice Stay and Hospitalization of Persons with Do-Not-
Hospitalize Order. The report says “Multiple TEP members described situations in which patients who had preferred not to be hospitalized changed their minds when a crisis occurred. Patients’ preferences and unexpected crises are usually out of the hospice’s control. Although it is still important for hospices to ask patients about their preferences as part of patient-centered care, the TEP did not believe these two items would be practical measures of a hospice’s care quality.”
Dr. McNally expects that Abt. Associates will apply the HQEP TEP’s suggestions to the HOPE tool.
“Oh yeah, they did it,” he says. “Abt would come to a specific meeting with information, data, suggestions, and specific information about how these things would be measured. We’d give feedback. Then they’d come back to the next meeting having incorporated our suggestions,” he explains. “All of us felt very much heard and responded to. It didn’t feel in the least bit perfunctory.”
Whatever specific measures are eventually included in the HOPE tool, Lund Person sees value in its implementation. “Hospice providers have had a woeful lack of outcome measures for hospice patients, which has made the evaluation of quality hospice care based only on process measures and the family’s evaluation of hospice care in the CAHPS® Hospice Survey, she explains. “Implementing HOPE will begin to identify outcome measures that can be compared between providers.”
Lund Person warns of potential challenges as well. “The selection of risk adjustment and stratification must be carefully done to minimize bias and maximize effectiveness of measures,” she says. “In addition, hospice providers have been awaiting the release of the HOPE tool with significant anxiety about content and administrative burden.”
Dr. McNally is confident the HOPE tool will be a healthy change for hospices.
“A lot of my role as a medical director and hospice physician is supporting our nurses,” he says. “They do 95% of the work. I really would like to see this not be burdensome for our hospice nurses. I’m looking forward to seeing what the [HOPE tool] beta testing translates to in our own hospice world.” He added “What I would hope to see is that the tool feels user-friendly to the hospice team, the people who have to use it, and that it also provides useful information to patients and families.”
NAHC’s Wehri says that standardizing processes through the HOPE tool is the key foundational element for the hospice industry. “High quality care is driven by reducing variance through standardized processes, Wehri writes. “Also, CMS will have a better idea of how the type of population a hospice serves impacts some of the clinical care.” This small glimpse into hospice variances that CMS does not currently have could be very helpful in future policy and payment decisions, according to Wehri. “What CMS finds in terms of differences between hospices and their care for patients may be a bit of a surprise to CMS,” she says. “I hope they are pleasantly surprised with the overall quality of care that is revealed.”
# # #
 Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.
Beth Noyce provides education, consulting, mentoring, compliance assessments and auditing services to home health and hospice agencies and their clinicians in several states. She also now provides patient and family guidance concerning hospice and home health services. Beth loves teaching and helping others succeed. She also makes available recordings of much of her education for her clients’ convenience.
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com
by Rowan Report | Apr 18, 2024 | Clinical, CMS, Regulatory
by Beth Noyce, RN, BSJMC, HCS-C, BCHH-C, COQS
CHAP-certified home health & hospice consultant
Process Measures
The outcome measures being considered look at effectiveness of hospice clinical efforts to decrease pain and other symptoms. The process measures paired with them focus on the hospice’s follow up with the patient after moderate or severe symptoms are found during assessment.
Exhibit 6 (below) shows the numerator and denominator for these.
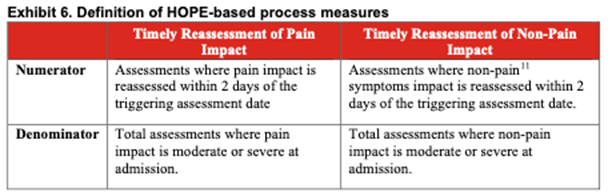
TEP members determined that these two process measures have high face validity. This means the measure items clearly state, or “look like” they will measure what CMS intends them to measure. This allows consumers to see what hospices are assessing and treating. It can also help hospices track how well they are reducing or treating patients’ symptoms.
Katie Wehri, Director of Home Health & Hospice Regulatory Affairs for the National Association for Home Care & Hospice says the face validity of process items is the most important information the HQRP TEP provided to CMS. “Having HOPE items and subsequent measures that actually measure what is intended is key to success,” she says.
Exclusions from Process Measures Success
Exclusions from calculating a hospice’s process measures’ success need careful consideration. Here is the list of options of which patients to exclude:
- Patient desired tolerance level for symptoms
- Patient preferences for symptom management
- Neuropathic pain
- Actively Dying (death is imminent)
- Other conditions
The report says that reassessing a symptom within two days of identifying that symptom as moderate or severe is fundamental. This is true regardless of the beneficiary’s stated tolerance-level for symptoms. It also said that process measure calculations should include patients with no symptom-management preference. Further, exclusion criteria should be the same for pain and non-pain symptoms.
Neuropathic Pain
The TEP’s recommends including neuropathic pain in the HOPE tool’s pain-reassessment process measure. Including rather than excluding patients suffering neuropathic pain prompts nurses to reassess these patients for changes. The report references research that suggests 40% of hospice patients may experience neuropathic pain. Patients who experience neuropathic pain have more severe and more distressing pain symptoms. [Tofthagen, C., Visovsky, C., Dominic, S., & McMillan, S. (2019). Neuropathic symptoms, physical and emotional well-being, and quality of life at the end of life. Supportive Care in Cancer, 27(9), 3357-3364. doi:10.1007/s00520-018-4627-x]
The TEP agrees that patients with neuropathic pain should be part of the process measure. However, they recommend excluding the same patients from the outcome measure addressing the patient’s pain impact. The report cited TEP discussion that such pain is chronic and not likely to be resolved or decreased within two days when the reassessment captures outcome data.
The TEP broadly agreed that a nurse who assesses a patient who is actively dying (life expectancy of 3 days or fewer based on clinicians’ assessment) as suffering moderate or severe pain should attempt to reassess the patient. Such patientsshould not be excluded.
The panelists agreed that process measures should include patients of all ages. Several TEP members noted that all patients experience pain and non-pain symptoms, and therefore the measures should apply to adults and children alike.
Exclusion Due to Inability to Reassess
When a hospice is unable to reassess a patient for a valid reason process measures should exclude those patients.
Identified exclusion reason were:
- discharge, alive or dead
- visit refusal
- inability to access the patient due to an emergency department or hospitalization event
- the patient traveling outside of the hospice’s service area
- inability of the hospice to contact the patient or caregiver.
However, the report says, “…hospices should be penalized if reassessment is missing or delayed due to hospice staffing or scheduling issues.”
This article is the second in a series about implementation of HOPE. Next week, Beth Noyce shares details from the panel as it discussed potential future process and outcome measure concepts.
# # #
©2024 by The Rowan Report, Peoria, AZ. All rights reserved. This article originally appeared in Healthcare at Home: The Rowan Report. One copy may be printed for personal use: further reproduction by permission only. editor@therowanreport.com











