In October of 2023, nurse Joyce Grayson went to the home (halfway house) of a released convict. She was later found dead in the basement of the house. In addition to adding focus to home care worker safety, the immediate response to this tragic event was an increase in nurses being afraid to do their jobs. Lawmakers in Connecticut vowed to increase protection for visiting nurses to ensure health care worker safety. The nurses requested additional reporting requirements for assaults while lawmakers suggested requiring an escort for high-risk situations.
Home Care Worker Safety by Law
Connecticut Senator Saud Anwar recognizes the growing segment of people wanting to age at home. “We want people to be able to get treatment at home,” he said. However, he also recognized the need for more information about potentially dangerous homes. He said at-home health care workers should be aware of what they’re walkin into “if there’s a high-risk situation.” Conn. lawmakers introduced Senate Bill One for Session Year 2024. The bill would require agencies to provide patient information, as applicable, including:
Medical History
Psychiatric history
History of violence
History of substance abuse
History of domestic abuse,
Current infections and treatments
Stability of diagnoses or symptoms over time
Housing Information
Other persons in the home
Name and relationship to patient
Psychiatric history
History of violence or domestic violence
Criminal records
History of substance abuse
Location of Service
Crime rate
Presence of hazardous materials
Presence of firearms or other weapons
Status of location’s fire alarm system
Presence of any other safety hazards
The bill also included ongoing safety training, safety assessments, and safety checks including:
A mobile app with patient information
A GPS enabled wearable device that allows staff to contact law enforcement
The Bill included payment rates to offset the cost of implementing all safety items to ensure cost-neutrality.
Implications for Hospice Agencies
Barbara Pearce, interim CEO of Connecticut Hospice, raised some legitimate concerns over the bill. Pearce warns that the background screenings required are lengthy and would result in many patients not receiving hospice care at all. According to Pearce, Connecticut Hospice “had 300 people die within three days, 200 people within two days, and 100 people within one day of entering home hospice care.” None of these patients would have been cared for if the bill had been in place at the time. Pearce discussed her concerns with Conn. lawmakers, who have since changed their approach.
Senate Bill One "Home Care Worker Safety" Moving Forward
Connecticut lawmakers are opting to exclude hospices from the bill for now. Sen Anwar said they plan to write a hospice-tailored bill “in the future” to ensure safety of hospice workers. Anwar continued, “We will have a plan of action to see what can be done to reduce the risk for hospice care workers too because…we want to make sure they’re safe too.”
The Connecticut 2024 legislative session is scheduled to adjourn on May 8. Senate and House representatives are racing the clock to modify the bill before the session ends.
Implication for Home Health
Few, if any, states have laws for home health worker safety. Alaska and Idaho have strict penalties for violence against health care workers. Wyoming introduced a similar bill in 2013, but it was defeated. Oregon passed a law in 2007 to require hospitals and surgery centers to implement safety strategies. Washington state established a law in 1999 that requires the development and implementation of a work-place violence plan. The law includes home health, hospice, and home care agencies, but does not have the detailed measures included in Connecticut’s bill.
If Senate Bill One passes in Connecticut, it could pave the way for additional state or federal regulations for in-home care safety precautions. Violence in home health, hospice, and home care has increased and steps need to be taken to ensure the safety and well-being of caregivers. Keep an eye out for some upcoming product reviews on mobile apps and hand-held emergency devices that allow home care workers to alert the agency, law enforcement, and/or family members before, during, and after a care visit.
# # #
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
A key purpose of the Health Insurance Portability and Accountability Act (HIPAA) is certainly to protect patient information. Another is to help ensure that patients have access to their health information. In fact, the Office of Civil Rights (OCR) of the U.S. Department of Health and Human Services, the primary enforcer of HIPAA, has focused on enforcement actions against providers that do not make information available to patients on a timely basis. OCR launched a right to access enforcement initiative in 2019 that is continuing.
Providers must give medical information to patients and their representatives within thirty days of requests. When they fail to do so, they may be subject to enforcement action by OCR. Following are two examples of recent enforcement actions.
OCR announced on April 1, 2024, that Essex Residential Care in New Jersey will pay a civil money penalty of $100,000 to resolve violation of HIPAA’s right of access standard. This is the 48th settlement reached under the right of access initiative. OCR received a complaint in May of 2020 from the personal representative of the estate of a patient who passed away. Following an investigation by OCR, the personal representative, who was the son of the patient, received the records in November of 2020. The provider did not contest the fine.
In another recent case, the daughter of a patient who passed away was appointed as the personal representative of her mother’s estate. She made multiple requests to Phoenix Healthcare for a copy of her mother’s medical records. She finally received the records one year after her initial request. Phoenix Healthcare initially received a civil money penalty of $250,000 for failure to provide timely access.
The provider appealed. An administrative law judge (ALJ) upheld the violation and ordered Phoenix to pay a civil money penalty of $75,000. The Departmental Appeals Board affirmed the ALJ’s decision. Then Phoenix agreed to settle for $35,000 and waived the right to further appeals. While it may seem in this case that the provider’s appeals significantly lowered its costs, it is important to note that the provider also undoubtedly expended significant resources on two appeals of OCR’s enforcement action.
Providers have placed a great deal of time and effort into the protection of healthcare information in compliance with HIPAA. Rightfully so, but providers seem to have lost sight of the fact that HIPAA is also about ensuring that patients and their representatives have timely access to their records. Now is the time for providers to conduct intensive education of staff members about HIPAA’s requirements regarding access in order to avoid enforcement actions like those described above.
For a few weeks now, we have been covering the Change Healthcare cyberattack by ALPHV/BlackCat and the subsequent updates from CMS. Pharmacy and medical orders have been delayed, providers and patients are suffering, and CMS has issued “guidance” with no real solution. Underground reports indicate that Change Healthcare paid $22 million to BlackCat following the first cyberattack and that BlackCat stole 6TB of data from the system. Change Healthcare has refused to respond to questions about the alleged payment. Three weeks after the attack, Change Healthcare started to come back online, starting with the pharmacy services, which returned on March 7th. Parent company UnitedHealth Group indicated that other services would return in the coming weeks.
Legal Action
More than 87% of physicians are see more than a 20% drop in daily claim submissions. As of April 9th, physicians are still reporting issues with cash flow and anticipate higher than expected losses due to financing and loans that may be needed to cover them as the effects of the attack continue. Rivals of Change Healthcare are reportedly onboarding hundreds of customers who have left the organization. One of these, Availity, has processed more than $5 billion in claims that were left unprocessed by Change Healthcare’s system and has onboarded 300,000 providers with a backlog of more than 50 health systems waiting to start using the platform.
The attack has caused long-term disruptions, delays, cash flow problems, patient care disruptions, prescription delays, and billing issues. Some physician practices have started using personal money to cover payroll and other expenses. The US Department of Health and Human Services (HHS) has launched a formal inquiry into Change Healthcare’s data protection standards. This inquiry follows six class action lawsuits filed against the organizations. Physicians were still reporting significant impacts on their claims.
Adding Insult to Injury
Change Healthcare has barely gotten their systems up and running were still putting out fires when they were hit again. On April 8, RansomHub contacted Change Healthcare and alleged to have 4TB of data stolen from the system and are demanding an extortion payment to keep the data private . RansomHub has threatened to sell the data, which includes US military personnel and patient data, medical records, and financial data, to the highest bidder in 12 days if the ransom isn’t paid.
Among the prevailing theories as to why Change Healthcare has been hit again is that the first ransom was supposed to have been split between ALPHV/BlackCat and an associate known as “notchy”, but ALPHV absconded with the ransom, leaving the other with nothing. Looking for a payout equal to what they lost, notchy partnered with RansomHub to try to recoup their losses. A second theory is that ALPHV and RansomHub are one in the same and that ALPHV went to ground after the ransom payout and have resurfaced as RansomHub. RansomHub, however, claims that after ALPHV went to ground, some of their affiliates joined the RansomHub operation and this is how they came by the data. Either way, it seems that the data stolen in the first attack was not returned after the ransom was paid and Change Healthcare is still susceptible to further extortion. This also means that the Change Healthcare system was not hacked a second time, but rather this is just an extension of the first data breach.
No word yet on whether Change Healthcare and UnitedHealth Group will pay the second ransom demand.
We will continue to follow this story and provide updates as it impacts payment and claims processing.
# # #
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
By Beth Noyce, RN, BSJMC, HCS-C, BCHH-C, COQS Home health & hospice consultant
The Hospice Outcome Patient Evaluation is a step closer to implementation.
After four years of considering options, the Technical Expert Panel (TEP) has finished its work that will inform future Hospice Quality Reporting Program results. The TEP considered quality measures to include in hospice’s future assessment tool and best choices for risk adjustment and exclusion.
The panel convened in 2019 “[we are] committed to improving the quality of care given to hospice patients,” says the 2022-2023 TEP Summary Report: Hospice Quality Reporting Program. The panel aimed to ensure that hospice quality measures are meaningful for hospice beneficiaries, transparent to hospice providers, and useful to consumers. They considered quality measures from both HOPE and claims data.
“From day one it was very clear Medicare wanted to make this a very different experience for hospice teams and make it a more valuable thing for consumers,” says Dr. Jeff McNally, Hospice Medical Director at Utah’s Intermountain Hospice,” describing his participation on the HQRP TEP. “I was actually encouraged and inspired by it,” he says. “It was the first time I had first-hand experience working with any kind of CMS entity.
“The reality is some clinicians in the field and leaders don’t have the best things to say about CMS,” he explains, but “whatever we were considering we always circled back to whether it would be burdensome to the clinical team and would it be valuable to consumers.”
The panel initially planned to meet multiple times in person, with two meetings per year and potential virtual meetings as needed. “Then COVID hit,” Dr. McNally says. “It slowed the process considerably. We never did meet again in person.”
The HQRP TEP met eight times over four years, virtually after the initial meeting. McNally described participants as coming to each meeting prepared with data and proposals for HOPE measures for which they would request input from panelists.”
From TEP recommendations early in their work, Abt Associates developed two outcome measures and two process measures in harmony with hospice’s central tenet to manage symptoms:
Process measures:
Timely Reassessment of Pain Impact
Timely Reassessment of Non-Pain Symptom Impact
Outcome measures:
Timely Reduction of Pain Symptom Impact
Timely Reduction of Non-Pain Symptom Impact
“The most important [recommendations] were some of the outcome measures about symptom management,” McNally explains. “What should we be helping agencies show that they’re doing well? And how do we do that? Deciding which ones, and how many symptom management measures to use and the most valuable way to show it in a fair way.”
During the past two years, TEP members prioritized which of the risk-adjustment factors suggested by Abt. Associates should apply to outcome measures and which exclusions should apply to both outcome and process measures.
The report describes risk adjustment as using statistics to exclude “confounding factors,” or elements that are outside of a hospice’s control, from calculations that could make a hospice’s performance appear either better or worse than it is. In essence, risk adjustment increases the fairness in outcome-measure calculations while exclusions do the same for both outcome and process measures.
For the outcome measures being considered, the report says that the “TEP broadly agreed that risk adjustment is very important because it accounts for external factors outside hospices’ control and more accurately reflects the quality of care provided.”
Judi Lund Person, Principal of LundPerson & Associates, LLC, agrees. “The discussion of risk-adjustment factors is vitally important to the success of upcoming process measure implementation,” says Lund Person.
Determining which risk-adjustment factors to bring to the table was not easy. “There were some nuance things that we hashed out to try and decide how to weigh some factors in risk adjustment” for outcome measures, McNally explains.
Exhibit 5 (below) summarizes the TEP’s rankings of risk adjustors suggested.
While the TEP’s priorities seem clear, the discussion concerning each risk adjustor was more complex. The TEP broadly agreed that the most important risk-adjustment factors are age and diagnosis. Some diseases are more difficult to manage than others, and patient condition tends to decline with age regardless of provider activity. Therefore, the TEP recommended that CMS adjust for these factors to ensure that common external factors do not adversely affect reported hospice care quality.
Here’s part of the nuance – the TEP also raised concerns that how well other patients with certain diseases or of certain age groups are treated might be valuable to some patients and their families seeking care for someone of the same age group or condition. Panelists fretted over possibly obscuring that information for consumers seeking hospice care by adjusting for those risk factors.
Living situation as a risk adjustor ranked as important to TEP members because hospices have no control over what level of assistance is available to patients. Similarly, site of service ranked high as a risk adjustor because, said some panelists, care is delivered very differently across settings, and patients and/or caregivers tend to provide higher hospice satisfaction ratings for hospices in home settings than for those in facilities,” according to the report.
Lund Person, who is also former Vice President of Regulatory and Compliance at the National Hospice and Palliative Care Organization (NHPCO), notes that the TEP recognized living situation and site of service as “important” risk adjustment recommendations.
“Identifying site of service will help to distinguish between care at home and care in a facility,” she says. Also vital, she continues, “is the recommendation from the TEP to consider length-of-stay as a risk-adjustment factor, including the differences between a 4-day length of stay and a 6-month length of stay.”
One TEP member cautioned that using payment sources, IV therapy, and risk of hospitalization as risk adjustors might tempt some hospices to use them to distort a hospices’ apparent care quality.
TEP members did not recommend using as risk adjustors gender, clinical symptoms, functional status and management of care needs. They did not discuss why they rejected gender, but several agreed that using clinical symptoms would not be of value because of their high correlation with diagnoses. Because hospice providers typically see hospice patients decline in ADL and IADL abilities, and hospice goals are focused on comfort rather than functional improvement, functional status was on the TEP’s “Do Not Include” as a risk adjustor list. And finally, one TEP member strongly opposed adjusting for patients’ medication management, supervision or safety assistance needs (management of care needs), explaining that “the public and CMS should hold hospices accountable for planning around oral medication, injectable medication management, and supervision and safety assistance,” the report says.
The TEP did suggest that using some risk adjustment factors as part of the HQRP could assist hospices internally with quality improvement while others would be more valuable to patients and families. For example, Patients and families would benefit from more straightforward risk adjustment that helps them select a hospice,” the report says, “including factors such as diagnosis. For publicly reported data used to select a hospice, the TEP suggested using demographic factors (including age but excluding gender), socioeconomic factors, living situation, and diagnoses.”
Dr. McNally hopes eventually to use HPRP data to promote Intermountain Hospice’s care. Intermountain Hospice is part of Intermountain Health, a health care provider with presence in multiple states. “You can’t take the current metrics to doctors’ offices and families to show anything meaningful,” he says. “It’d be great to have metrics we could take to our neurology docs and other docs,” he says. “I really think we provide better care and more options when patients stay within our system.
This article is the first in a series about implementation of HOPE. Next week, Beth Noyce shares details from the panel as it evaluated process measures.
In 2020, doctors flooded telehealth companies with requests for help caring for patients reluctant to leave home to come to their appointments. Following suit, many Home Health agencies that had never considered investing in home telehealth before, opened up their wallets to acquire equipment, from simple wearables to high-end, HIPAA-compliant video systems.
In addition to the need to provide care at a safe distance, many HHA leaders knew the added service would attract the attention of hospitals desperate to discharge recovering Covid victims as well as non-Covid patients. Some HHAs established relationships with hospitals they had not had before, given the chance to demonstration Home Health’s unique advantages over extended hospital stays and discharges to institutions such as SNFs that had become virtual death sentences during the height of the pandemic.
All Things Must Pass
With the introduction and widespread free availability of Covid mRNA vaccines, the death rate graph line began to tilt downward. Then came the discovery that the SARS-CoV-2 and its variants are transmitted through the air and not through unwashed surfaces. People stopped disinfecting their counter tops after unloading groceries. And they started in-person doctor visits again. Patients returned to allowing nurses into their homes.
In regions where vaccination and booster rates were high, hospitals found themselves with more and more empty beds. They took down tented treatment centers in their parking lots and sent refrigerated trailers back to trucking companies. Desperation referrals to Home Health tapered off, as did the need for virtual visits.
Isaac Newton said every action has an equal and opposite reaction. If that holds true in the healthcare business as it does in physics, the reaction to Covid easing is seen in Remote Patient Monitoring tech companies. According to Fierce Healthcare, the New York Stock Exchange told one RPM company, Amwell, formerly known as “American Well,” to raise its stock price or be delisted. Fierce added detail about the company’s woes:
“Despite decimating its workforce at the end of 2023 to cut expenses, the company still projects a 2024 loss between $160 million and $155 million amid incremental revenue growth. The company’s market cap was a stone’s throw from $6 billion at the height of its valuation, when shares were trading for more than $42 each. Amwell shares were trading at $0.72 as of market close on April 5, giving the company a current market cap of about $208.6 million.
Another market leader fared no better, Fierce Healthcare found. “Telehealth giant Teledoc, which has been in operation for 20 years, has struggled in the stock market and is facing headwinds as the virtual care market has become crowded with digital health players. Shares dropped 22 percent in February as the company missed fourth-quarter revenue estimates and offered a downbeat forecast for the rest of the year.”
Teledoc’s 15-year CEO, Jason Gorevic, resigned last week after the company reported a net loss of $220 million for 2023, following 2022’s historic loss of $13.7 billion, mostly from a write-off related to the plummeting value of its ill-advised Livongo acquisition. According to Fierce Healthcare, Teladoc shelled out $18.5 billion for the digital chronic condition management company, a record in digital health.
Gorevic’s rationale that the telehealth field has become too crowded may not be far off. Last July, Becker’s Hospital Review published an industry survey titled “280+ Telehealth Companies to Know.” The list included a half dozen names we recognized from past Home Health conferences, including Health Recovery Solutions, AMC, Vivify, and FoneMed.
Do Hospital Woes Translate Down to Home Health?
Making comparisons between telemedicine companies that focus on hospitals and physicians and those who focus on post-acute providers is hampered by the fact that few in our sector are publicly traded and do not share their numbers. UnitedHealth, which acquired Vivify in 2019 and assigned it to its Optum division, does not separately report Vivify revenue.
Health Recovery Solutions, one of the best-known names in post-acute RPM, is privately held by its founding CEO and seven investors. Its most recent influx of $800,000 occurred in January, 2022, making it impossible to determine whether it was motivated by investor confidence or the need for cash as Covid began its decline.
Analysis
This publication has promoted the advantages of remote patient monitoring for its entire 25-year existence. We have covered startups and established tech companies offering every technology from PERS to Zo monitors to automated phone calls, in-home cameras and microphones. We have followed the evolution of two-way communications and vital sign detectors from tabletop devices to tablets and smartphones. We have even tested a few robots. We have seen HHAs experience great success, and we have seen devices collecting dust on shelves.
Throughout, we have maintained that, when selected, implemented, and deployed properly, monitoring patients 24/7 instead of once or twice a week can improve patient outcomes, boost agency reputation, and, more often than not, produce a healthy ROI. The end of the latest pandemic may mean the end of demand for Remote Patient Monitoring systems, but that would be unfortunate.
Tim Rowan is a 30-year home care technology consultant who co-founded and served as Editor and principal writer of this publication for 25 years. He continues to occasionally contribute news and analysis articles under The Rowan Report’s new ownership. He also continues to work part-time as a Home Care recruiting and retention consultant. More information: RowanResources.com or Tim@RowanResources.com
HealthRev Partners Launches Velocity as a SAAS, Transforming Revenue Cycle Management for the Home Health and Hospice Industry
Meta: Discover how HealthRev Partners’ innovative SAAS solution, Velocity, is transforming revenue cycle management in the healthcare industry. Gain insights into its key advantages, AI capabilities, and data exchange interface engine feature set. Learn how Velocity empowers agencies with transparency, efficiency, scalability, and security to enhance profitability and operational excellence. Contact HealthRev Partners for a demo and revolutionize your revenue cycle management today.
Ozark, MO – April 1st, 2024 – HealthRev Partners, a leading innovator in healthcare technology, has announced the launch of Velocity as a Software as a Service (SAAS), revolutionizing revenue cycle management in the home health, hospice, and palliative care industries. This game-changing solution is designed to transform revenue cycle management (RCM) for multi-site agencies. In an era where the aging population in America increasingly desires to age in place, mergers and acquisitions in the home health space are driving the necessity for centralized data and operational processes. The trend of overseas hiring to reduce costs has created gaps in insights, emphasizing the critical need for real-time data to impact care promptly.
Michael Greenlee, Founder and CEO of HealthRev Partners, expressed his enthusiasm about the launch, stating, “Velocity as a SAAS represents a significant leap forward in revenue cycle management technology. By offering agencies unprecedented insights into their operations and empowering them with tools for optimization and growth, HealthRev Partners is setting a new standard in RCM solutions.”
Empowering Multi-Site Agencies and Enhancing Management Insights
As multi-site agencies navigate the complexities of managing diverse locations and teams, the demand for comprehensive insights and seamless integration becomes critical. HealthRev Partners recognizes this challenge and introduces Velocity as a SAAS to address the evolving needs of growing agencies. With a focus on providing real-time analytics and enhancing operational efficiency, Velocity bridges the gap between disparate locations and centralizes data for streamlined management.
Seamless Integration with Any EHR System
A key component of Velocity is the data exchange interface engine feature set. The ability to connect, integrate, translate, and import financial, claims, coding, clinical, operational, EHR, clearinghouse, and diverse data sets is vital for any organization. Velocity uses its proprietary interface technology engine along with robotic processing technology (RPA) to connect all disparate data sets within Velocity resulting in actionable data at your fingertips.
AI Capabilities to Increase Coding Accuracy
Velocity harnesses AI capabilities to automatically assign charts to coding professionals, enhancing efficiency and accuracy. By leveraging artificial intelligence, it streamlines the ICD-10 coding process and provides intelligent suggestions for selecting codes at the highest level of specificity to maximize reimbursement. Additionally, it utilizes advanced algorithms to analyze data and offer insights into PDGM-approved primary codes and comorbidity adjustment categories. Furthermore, Velocity’s AI-driven system assists in risk and comorbidity adjustments by recommending compatible code combinations and presenting primary and secondary code sets to facilitate precise coding decisions.
Key Advantages of Velocity:
Increased Transparency and Visibility: Real-time insights into all aspects of the revenue cycle across multiple sites. Identify bottlenecks, track productivity, and optimize operations seamlessly.
Enhanced Efficiency and Accuracy: Streamlined processes and standardized procedures that ensure consistency across all locations. Improve accuracy in coding, claim submission, and reimbursement.
Improved Communication and Collaboration: Facilitate real-time data sharing between clinical, financial, and operational teams at different sites. Enhance collaboration and decision-making.
Scalability and Security: Easily scale operations to accommodate growth needs while maintaining top-tier data security standards. Ensure compliance with regulatory requirements across all locations.
Michelle Mullins, MHA, BSN, RN – Partner & Chief Operating Officer of HealthRev Partners, highlighted the transformative impact of Velocity by stating, “Velocity illuminates your RCM’s path to predictable revenue. It empowers agencies with granular insights, customizable control, streamlined operations, and trustworthy security. This tool is not just a solution; it’s a revolution in revenue cycle management.”
The launch of Velocity as a SAAS marks a pivotal moment for agencies seeking to optimize their revenue cycle processes. With its focus on transparency, efficiency, communication, scalability, and security features, Velocity is poised to reshape how agencies manage their RCM operations.
# # #
For more information about Velocity as a SAAS or to schedule a demo, visit HealthRev Partners’ website.https://healthrevpartners.com/
On March 28, CMS issued a new proposed rule to update Medicare hospice payments. Here’s what we know.
The new proposed rule:
Would change the existing hospice wage index
Clarifies current policy related to the hospice “eletion statement” and the “ntoice of election”
Adds clarifying language around hospice certification
Includes a request for information to get comments on implementing a separate payment mechanism for high-intensity palliative care services
Proposes that Hospice Quality Reporting Program (HQRP) measures be collected through the Hospice Outcomes and Patient Evaluation (HOPE), adding two new measures
Also proposes changes to the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Hospice Survey
The new proposed rule includes a net 2.6% increase in payments over FY 2024. This includes a 3% market-based update, and a 0.4% cut for productivity. Submitting quality data is a requirement of the net pay. Hospices that do not submit quality data will be penalized 4%, netting a 1.4% decrease in payments. The propsed rule for 2025 is .5% lower than the 2024 hospice payment increase.
The National Hospice and Palliative Care Organization (NHPCO) says the rate increase is good, but not high enough. NHPCO COO and Interim CEO, Ben Marcantonio said, “To continue providing the high level of care our patients and their families deserve, hospices require a payment rate that accurately reflects the current economic challenges. We know that hospice care has demonstrated $3.5 billion in annual savings for Medicare, which underscores the critical importance of investing in hospice to ensure continued beneficiary access to quality end-of-life care.”
Palliative Care
CMS is interested in feedback and proposals from hospice agencies for providing complex palliative treatments and high-intensity hospice care when that care negatively impacts hospices financially. CMS aims to care for high-cost patients through palliative care rather than acute care. The NHPCO agrees with the CMS proposal to fund palliative care separately from standard hospice or acute care. CMS will take feedback and proposals through May 28, 2024. Comments can be submitted electronically at http://www.regulations.gov, by following the “Submit a Comment” instructions. Comments can also be sent by regular or express mail. Addresses can be found in the full proposed rule. Follow the search instructions at http://www.regulations.gov to see all submitted comments.
Kristin Rowan has been working at Healthcare at Home: The Rowan Report since 2008. She has a master’s degree in business administration and marketing and runs Girard Marketing Group, a multi-faceted boutique marketing firm specializing in event planning, sales, and marketing strategy. She has recently taken on the role of Editor of The Rowan Report and will add her voice to current Home Care topics as well as marketing tips for home care agencies. Connect with Kristin directly kristin@girardmarketinggroup.com or www.girardmarketinggroup.com
by Bryan Robinson, PH.D. Contributor author of Chained to the Desk in a Hybrid World: A Guide to Balance
April is National Stress Awareness Month with the goal of raising awareness of the impacts of stress. According to the American Psychiatric Association, 26% of respondents anticipate they will be more stressed in 2023 and their mental health will be worse. Two out of five adults ranked their mental health from “fair” to “poor.” When you have fewer stressors, you have increased emotional stability, better moods and overall superior health. This month is a time to pay special attention to how you can remain stress-free throughout your workday, and you can do that in very simple ways. You don’t have to quit your day job or even work fewer hours. You can continue your daily work routines while practicing stress reducers at the same time. The one thing you must do is have a stress awareness plan that you can practice at work.
A Stress Awareness Plan Keeps Job Stress At Bay
My 2023 New Years Resolution was to do one kind thing each day for someone—especially strangers. It has heightened my awareness of how important and easy it is to be kind to others without taking extra time. Plus, how simple it is to practice and how good it makes me feel (and hopefully the other person) in just minutes. A work stress awareness plan has the same effect. Here’s how it works. Simply choose one thing to commit to each day that you can accomplish in three to five minutes to mitigate stress during your workday.
A max of five minutes of chill a day can have mental and physical benefits to keep you engaged, calm and energized on the job. These short work breaks lead to higher job engagement and performance as well as better sleep, increased immunity, lower blood pressure, improved digestion and increased emotional well-being. In fact, research from scientists at North Carolina State University shows the value of what I call Microchillers or taking what the researchers call Microbreaks throughout the workday. These short breaks—I recommend five minutes or less—are effective energy management strategies as simple as stretching, walking up and down stairs, gazing out a window at nature, snacking or having a five minute mindful meditation.
Viventium Releases its 2024 Caregiver Onboarding Experience Report, Demonstrating a Need to Raise the Bar for Onboarding in the Post-Acute Care Industry
BERKELEY HEIGHTS, N.J., April 02, 2024 (GLOBE NEWSWIRE) — Viventium, the leading SaaS-based human capital management platform serving the post-acute care industry, released its 2024 Caregiver Onboarding Experience Report, a comprehensive research study analyzing survey responses from 175 post-acute care administrators and 220 caregivers. The report finds a shockingly low bar for what passes as a “good” onboarding experience in home-based and facility/community-based care, with strong indications that raising that bar could correlate to higher retention rates.
“Staffing shortages and high turnover rates within post-acute care are recurring issues in need of solutions,” said Navin Gupta, Viventium CEO. “Our research illuminates a crucial pathway towards addressing these persistent challenges, and it begins with onboarding.”
Findings point to post-acute care managers and administrators having a major impact on the steps their organization can take to better engage, motivate, and retain its caregiving staff.
“The study significantly advances our knowledge of what it takes to recruit and retain caregivers in today’s highly competitive workforce market. The onboarding process is fully within the control of the employer, and the study shows that doing it right pays dividends. Most notably, many of the elements of successful onboarding are simple improvements in the process that bring a real return on investment. I would encourage all of home care to learn from this study.”
About Viventium
Viventium provides a SaaS-based human capital management solution that is focused on the post-acute care industry. The company’s mission is to enrich the lives of caregivers through technology so they love going to work every day. By providing specialized software and expert guidance, Viventium helps its clients throughout the lifecycle of each caregiver. The company has clients in all 50 states and supports over 420,000 client employees each year.
Average 2023 hourly rate for home health aide increased 5.2%
Hourly per visit nurse rate decreased 1.6% with facility prices mixed
Washington and New Hampshire most expensive states for home health aides
illumifin’s comprehensive study provides insight which empowers consumers, insurers, and providers by benchmarking the prices of senior care.
WOODBURY, Minn., March 27, 2024 /PRNewswire/ — illumifin, the leading insurance administration and claims solution provider for long term care (LTC) insurance, has just released its 2023 Cost of Care study and comprehensive analysis. Now in its tenth year, this longitudinal study includes national, state and regional costs of various care services, spanning skilled nursing, adult day care, home health care and assisted living facilities.
illumifin’s Cost of Care study gathers tens of thousands of data points from care providers nationwide, with results normalized by the company’s in-house actuarial and data science teams. Insurers and financial services providers rely on this data for both forecasting and stakeholder education as well as informing customers and agents about national and regional cost variations. In addition, care providers benefit from understanding the market rates for services in their area. These insights are also accessible via illumifin’s What Care Costs website, which offers interactive maps and projection tools to sort, rank and evaluate average costs of LTC services across the US.
illumifin’s study found that the average hourly rate for a home health aide in 2023 was $30.62, an increase of 5.2 percent over the prior year. Meanwhile, the average per-visit rate for a registered nurse in 2023 was $147.72, a decrease of 1.6 percent over the prior year, potentially reflecting rates beginning to normalize post pandemic.
The research also shows facility prices were mixed. The average assisted living facility rates increased between 0.6 and 3.8 percent in 2023 depending on room type, reversing course from the pandemic where assisted living facility rates had been trending downward. However, skilled nursing facility rates experienced a small decrease in 2023 between 0.4 and 1.0 percent.
The most expensive states for home health aides were Washington and New Hampshire, whereas Mississippi and Louisiana were the least expensive. Meanwhile, the most expensive assisted living rates were found in New Hampshire and New Jersey, while the lowest assisted living prices were found in Alabama and Oklahoma.
“We are proud to leverage our 30 years of experience in senior care to provide actionable data for insurers, consumers, providers and financial institutions,” said Peter Goldstein, illumifin’s President and CEO. “Our focus remains on customer centric initiatives which assist in managing risk and planning for the future. Our Cost of Care survey has proven valuable to not only to our business partners but providing valuable knowledge to consumers and their families as they navigate the maze of service types when making care decisions.”
The study, interactive tool and data are available for use by insurers, providers and financial services firms. For more information regarding illumifin’s Cost of Care Study, please contact Jennifer Frost via email at jenniferfrost@illumifin.com.
About illumifin illumifin provides third party administration and technology services to individual and group insurers. The company, launched in 2021, blends insurance industry knowledge, technology leadership and operational execution to prepare insurers for the digital future. illumifin is a diverse, passionate and empowered team of insurance specialists committed to the growth and success of its customers. With illumifin, there’s a brighter future. Visit www.illumifin.com.
Contact: Chris Tofalli Chris Tofalli Public Relations, LLC 914-834-4334




 On April 8, RansomHub contacted Change Healthcare and alleged to have 4TB of data stolen from the system and are demanding an extortion payment to keep the data private . RansomHub has threatened to sell the data, which includes US military personnel and patient data, medical records, and financial data, to the highest bidder in 12 days if the ransom isn’t paid.
On April 8, RansomHub contacted Change Healthcare and alleged to have 4TB of data stolen from the system and are demanding an extortion payment to keep the data private . RansomHub has threatened to sell the data, which includes US military personnel and patient data, medical records, and financial data, to the highest bidder in 12 days if the ransom isn’t paid.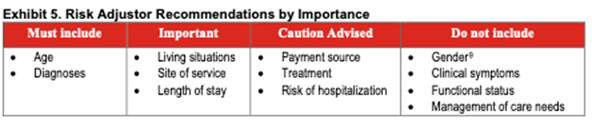
 With the introduction and widespread free availability of Covid mRNA vaccines, the death rate graph line began to tilt downward. Then came the discovery that the SARS-CoV-2 and its variants are transmitted through the air and not through unwashed surfaces. People stopped disinfecting their counter tops after unloading groceries. And they started in-person doctor visits again. Patients returned to allowing nurses into their homes.
With the introduction and widespread free availability of Covid mRNA vaccines, the death rate graph line began to tilt downward. Then came the discovery that the SARS-CoV-2 and its variants are transmitted through the air and not through unwashed surfaces. People stopped disinfecting their counter tops after unloading groceries. And they started in-person doctor visits again. Patients returned to allowing nurses into their homes. Making comparisons between telemedicine companies that focus on hospitals and physicians and those who focus on post-acute providers is hampered by the fact that few in our sector are publicly traded and do not share their numbers. UnitedHealth, which acquired Vivify in 2019 and assigned it to its Optum division, does not separately report Vivify revenue.
Making comparisons between telemedicine companies that focus on hospitals and physicians and those who focus on post-acute providers is hampered by the fact that few in our sector are publicly traded and do not share their numbers. UnitedHealth, which acquired Vivify in 2019 and assigned it to its Optum division, does not separately report Vivify revenue.

 April is
April is 

